Case of the Month ...
Case History
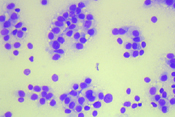
A 46 y/o woman with a thyroid mass. No history of thyroid disease and thyroid function tests are within normal limits. Ultrasound suggests a solid mass. A fine-needle aspiration is performed on the thyroid mass. (Figure 1 and 2)
Diagnosis & Discussion
click on image for larger version
DIAGNOSIS
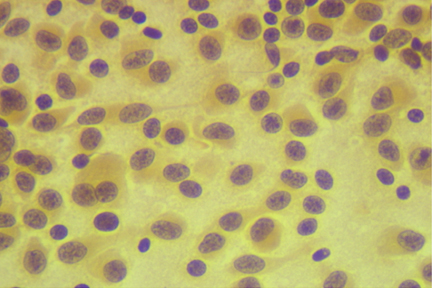
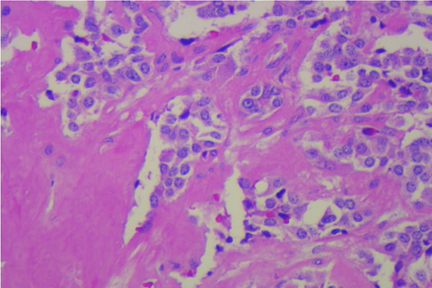
Medullary Carcinoma of Thyroid (Figure 3)
CYTOLOGY FINDINGS (Fig 1 and 2)
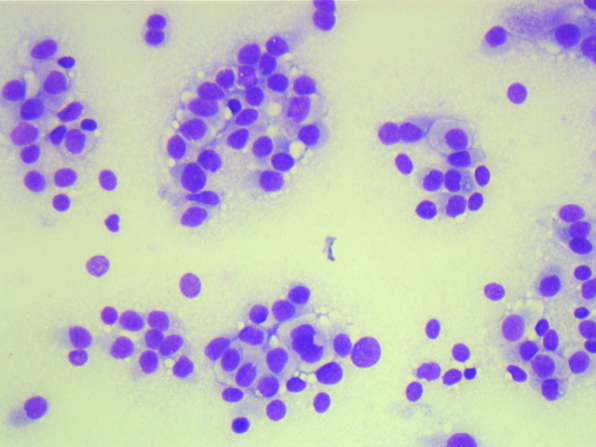
- Sparse colloid
- Cellular smear with plasmacytoid to spindloid monomorphic population of cells
- Cells tend to be dispersed
- Nuclear chromatin is speckled and dispersed
- Prominent nucleoli are not identified
- No definitive nuclear grooves or pseudonuclear inclusions
DIFFERENTIAL TO CONSIDER
- Plasmacytoid or spindle cells Medullary carcinoma of thyroid - Not the usual appearance of follicular cells nor are they extremely pleomorphic thus diminishing likelihood of the other primary types of thyroid carcinoma (papillary, follicular or anaplastic)
- Plasmacytoid lymphoma
- Sarcoma (extremely rare and usually more pleomorphic)
- Metastasis of other neuroendocrine or plasmacytoid neoplasm
DISCUSSION
Medullary carcinoma of the thyroid is an uncommon malignancy of the thyroid that tends to differentiate similar to the C-cells. The cells have the typical neuroendocrine appearance similar to carcinoid or neuroendocrine tumors of the pancreas with speckled chromatin (so-called “salt & pepper” chromatin) and a plasmacytoid to spindle cellular shape. They tend to secrete calcitonin which can be a useful ancillary monoclonal IP test as compares to papillary or follicular carcinoma of the thyroid that will be thyroglobulin positive and calcitonin negative. They are also associated with amyloid production that may be identified on FNA smears as amorphous background material but more often visible on the histology. Amyloid is Congo-Red stain positive with apple green birefringence when polarized but proper, even thickness is rarely obtainable on direct smears. Thus Congo Red staining may be less predictable than IP staining for cytology specimens. IP staining may also be performed on a smaller specimen quantity.
This form of thyroid carcinoma can have a familial tendency that can be evaluated by a blood test for RET protoncogene as a “germ-line” mutation. Recent diminished cost of this test along with the rarity of medullary carcinoma has prompted many clinicians to test all patients with the diagnosis of medullary carcinoma for this mutation. Positive RET in the patient would then lead to testing of blood relatives for preventative measures.
ACKNOWLEDGEMENT
This case is contributed by Dr. Larry Fowler from the Department of Pathology, University of Texas Health Science Center at San Antonio.