Case of the Month ...
Case History
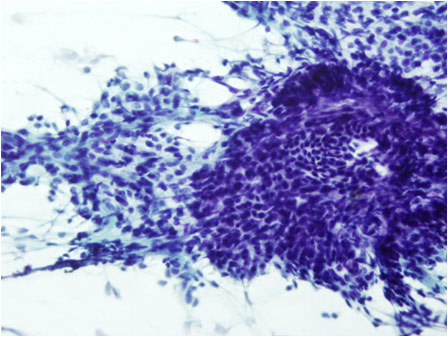
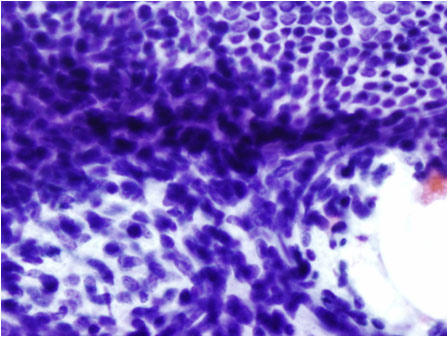
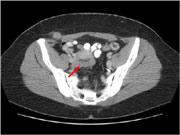
31-year-old female presented with a seven- month history of vague right lower abdominal pain. A CT scan of the abdomen revealed a 2 cm extraperitoneal soft tissue density in the region of the rectus sheath muscle concerning for a soft tissue tumor versus metastasis ( Figure 1 ). Her past history is insignificant except for a Cesarean section. An ultrasound guided FNA of the mass was performed. The Papanicalaou stained slide reveal a cellular smear consisting sheets and clusters of cells. (Figure 2) Two types of cells are noted. One type of cells appear bland and arrange in a honeycomb pattern.The nuclei of the second cell type displays round to oval and spindled shaped nuclei that are somewhat hyperchromatic and scant amount of non-descript cytoplasm. (Figure 3 and 4)
Diagnosis & Discussion
click on image for larger version
Diagnosis: Endometriosis at the incision site.
Discussion: Endometriosis of the skin and soft tissue tend to occur at sites of prior surgical scars resulting from the spillage of endometrial tissue during surgery. The incidence of endometriosis at the site of prior C-section scar is estimated to be less than 0.1%. They typically present 2-8 years later with nodules around the surgical tract. History of a slow growing mass with cyclical pain may be elicited.
Endometriosis needs to be differentiated from other benign and malignant lesions and for possible malignant transformation. The main differential diagnoses include metastatic well differentiated endometrioid adenocarcinoma, low grade endometrial stromal sarcoma and malignant mixed mullerian tumor.
The diagnosis of endometriosis is established by the triad of hemosiderin-laden macrophages, endometrial glands and spindle cell stroma. Unfortunately on cytology, all three components are rarely present and may erroneously suggest a purely glandular or spindle cell lesion. Presence of cytologic atypia may lead to a false diagnosis of a metastatic or primary endometrioid adenocarcinoma.
A primary or metastatic well-differentiated adenocarcinoma is usually composed of cellular clusters or sheets of small cells with a high nuclear to cytoplasmic ratio. Round to oval nuclei contain coarsely granular chromatin and small prominent nucleoli. Peripheral palisading at the edge of the cell clusters or squamous differentiation may occur. Most cases of endometrioid adenocarcinomas occur in the peri and postmenopausal women.
Low grade endometrial stromal sarcoma may mimic endometriosis especially if the sampling lacks an epithelial component. The smears are cellular composed of loosely packed monotonous cells. The cells have oval, normochromatic nuclei with smooth nuclear contours and small prominent nucleoli. An arborizing vasculature of small arterioles is suggestive of a stromal sarcoma.
Malignant mixed mullerian tumors (MMMTs) are biphasic tumors with epithelial and stromal components. They are usually cellular with a necrotic background. The epithelial component is usually pleomorphic and poorly differentiated. Heterologous elements like cartilage may be present. These tumors almost exclusively occur in postmenopausal women.
D 10 is a marker for normal and neoplastic endometrial stroma. In endometriosis, the glandular cells stain with cytokeratin while the endometrial stromal elements stain for CD10. It could also be used to confirm endometrial stromal sarcomas.
Follow Up: The FNA was followed by a core biopsy which was consistent with endometriosis.
Acknowledgement: This case is submitted by: Nalini Madiraju MD and Alaa Afify MD from the Department of Pathology, University of California, Davis, Medical center, Sacramento, CA.