Case of the Month ...
Case History
An 82-year-old Caucasian female presented to the Fine Needle Aspiration Clinic with a 3-year history of painless swelling in the vicinity of the right parotid gland. The patient denied any history of masses or lesions in this area or any recent trauma. A 2.5 cm soft, non-tender, tethered lesion was noted on physical examination superior to the angle of the right mandible.
Diagnosis & Discussion
click on image for larger version
Figure 1
Figure 5
Image Figures:
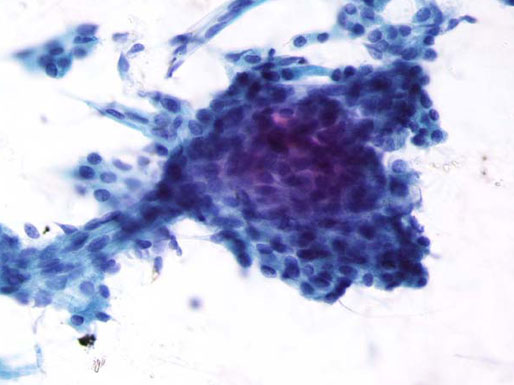
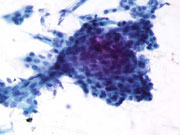
- FNA Cytology Smear (Pap stain) (Low magnification)
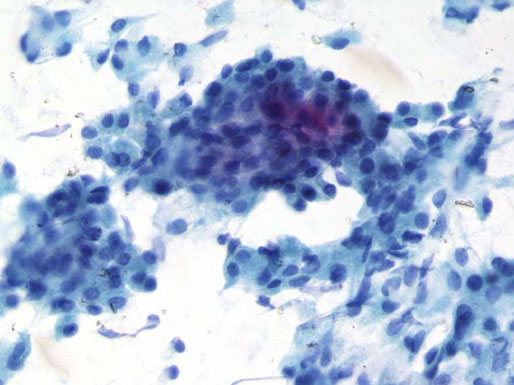
- FNA Cytology Smear (Pap stain) (High magnification)
- Cell block (H & E) (Low magnification)
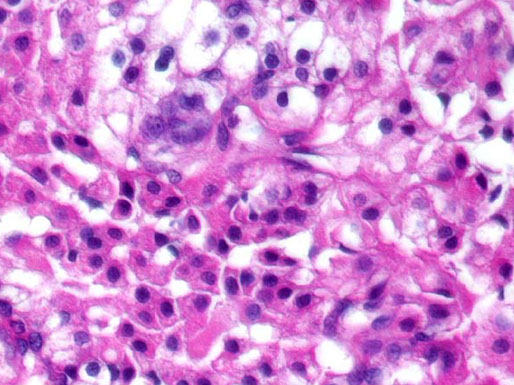
- Cell block ((H&E) (High magnification)
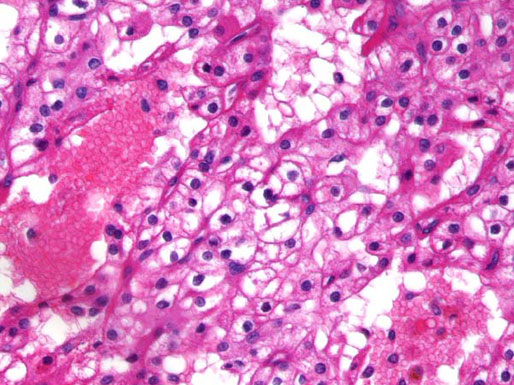
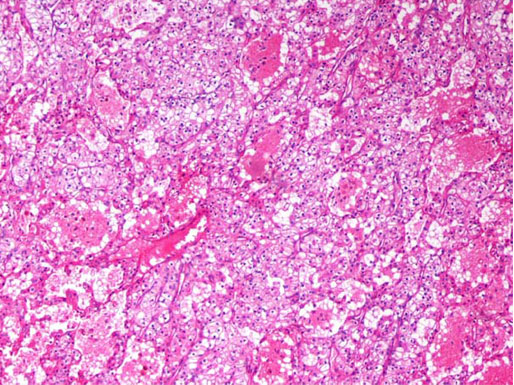
- Histologic Section (H&E)
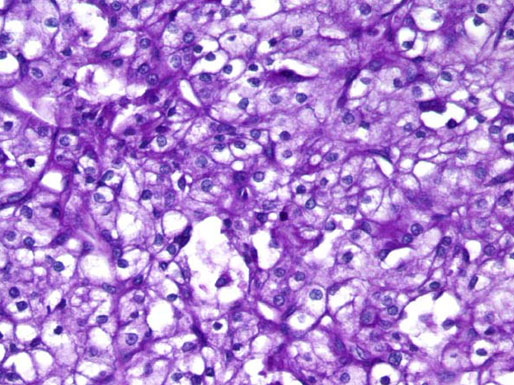
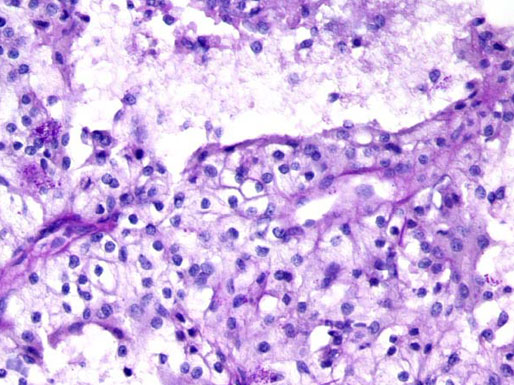
- Histologic Section (PAS without diastase)
- Histologic Section (PAS with diastase)
Diagnosis: Clear Cell Oncocytoma of Parotid Gland
Cytologic Findings:
- Polygonal cells occurring singly, in sheets and clusters
- Abundant clear to finely granular pale-blue to eosinophilic cytoplasm (Pap stain)
- Round to oval nuclei with moderately coarse chromatin and small nucleoli or chromocenters
- Polyhedral cells with intensely eosinophilic granular cytoplasm (H&E; Cell block)
Differential Diagnosis:
- Oncocytoma with clear cell features
- Epithelial-myoepithelial carcinoma
- Primary clear cell carcinoma
- Diffuse hyperplastic oncocytosis
- Metastatic renal cell carcinoma
- Clear cell Acinic carcinoma
- Mucoepidermoid carcinoma
- Clear cell change in Pleomorphic adenoma
- Polymorphous low-grade adenocarcinoma
- Sebaceous adenoma
Discussion: The salivary gland Oncocytoma is a rare tumor accounting for approximately 1% of all neoplasms in this organ. As in our index case, these tumors predominantly occur in middle-aged to elderly white females. The average age and duration of the lesion in one study was 57 (38 to 73 years old) and 6 months (4 months to 25 years), respectively. 1 Recurrence of the tumor following excision has been noted to occur in at least 20% of patients likely due to occult multifocality or incomplete excision. Oncocytomas grow in an expansile rather than infiltrative fashion, can occur bilaterally and usually contain a capsule. They are considered to be derived from normally occurring oncocytes in the aged parotid gland that over time become diffusely hyperplastic and form a well-circumscribed nodular lesion. The intensely eosinophilic staining cytoplasm is secondary to the presence of abundant mitochondria. The phosphotungstic acid-hematoxylin (PTAH) stain is useful in this instance to highlight their presence. The finding of abundant clear cells in an oncocytic tumor usually signifies either a fixation artifact, the accumulation of intracytoplasmic glycogen, margination of mitochondria and other cytoplasmic constituents or degenerative changes in cytoplasmic organelles. Intracytoplasmic glycogen is best detected using the Periodic acid-schiff (PAS) stain with and without diastase digestion. The May-Grünwald-Giemsa (MGG) stain can also be helpful in ruling out certain other cytoplasmic substances such as mucin and lipid. While fine-needle aspiration cytology has been shown to be very useful in accurately categorizing salivary gland neoplasms, a predominance of clear cells in aspiration material can be diagnostically challenging. As outlined above, clear cells have been observed in a number of tumors ranging from benign to low and high grade malignancies. The feature of optically clear cytoplasm, then, should warrant further work-up and investigational studies, such as excisional biopsy, to rule-out the presence of a more significant lesion.
References:
Ellis GL. “Clear cell” Oncocytoma of Salivary Gland. Hum Pathol 1988;19:862-867.
Ellis GL. Clear Cell Neoplasms in Salivary Glands: Clearly a Diagnostic Challenge. Ann Diagn Pathol 1998:2:61-78.
Layfield LJ, Glasgow BJ. Aspiration Cytology of Clear-Cell Lesions of the Parotid Gland: Morphologic Features and Differential Diagnosis. Diagn Cytopathol 1993;9:705-712.
Maiorano E, Altini M, Gianfranco F. Clear Cell Tumors of Salivary Glands, Jaws, and Oral Mucosa. Sem in Diagn Pathol 1997;14:203-212.
Davy CL, Dardrick I. , et al. Relationship of clear cell Oncocytoma to mitochondrial-rich (typical) Oncocytomas of parotid salivary gland (an ultrastructural study). Oral Surg Oral Med Oral Pathol 1994;77:469-78.
Mandel L, Carrao V. Bilateral Parotid Diffuse Hyperplastic Oncocytosis: Case Report. J Oral Maxillofac Surg 2005;63:560-562.
Capone RB, Ha PK , et al. Oncocytic neoplasms of the parotid gland: A 16-year institutional review. Otolaryngol Head Neck Surg 2002;126:657-662.
Hughes JH, Volk EE, et al. Pitfalls in Salivary Gland Fine-Needle Aspiration Cytology. Arch Pathol Lab Med 2005;129:26-31.
Acknowledgement: This case is contributed by Anthony A. Corsini, DO and Marina Mosunjac, MD from the Department of Pathology, Grady Memorial Hospital and Emory University , Atlanta GA