Case of the Month ...
Case History
A 48 year old Caucasian male presented for evaluation of abdominal fullness, slight epigastric pain and cough. No tenderness on palpation was noted. Routine laboratory tests failed to reveal any significant pathology. An abdominal CT scan was also performed as part of the diagnostic work up. The CT- scan demonstrated a 2.4 x 2.0 cm mass medial to the left kidney in the peri-renal space. The patient than underwent a CT-guided fine needle aspiration biopsy (FNA) of this mass.
Three months later, the patient returned complaining of the same symptoms. An esophagogastroduodenoscopy was performed which showed diffusely ulcerated and cobblestoned mucosa involving almost the entire length of the esophagus. The patient was started on empiric herpes simplex viral therapy for esophagitis. An esophageal brush specimen was submitted to cytology, and a corresponding biopsy was sent to surgical pathology.
Diagnosis & Discussion
click on image for larger version
Figure 1
Image Figures:
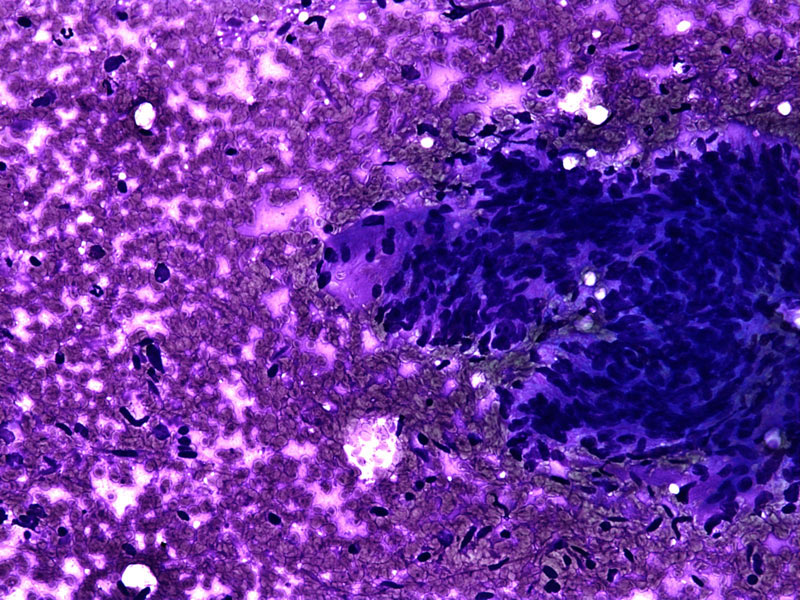
- Figure 1: FNA cytology smear, Diff-Quick stain, X 200
- Figure 2: FNA cytology smear, Papanicolaou stain, X 100
- Figure 3: FNA cytology smear, Papanicolaou stain, X 200
- Figure 4: FNA cytology smear, Papanicolaou stain, X 400
- Figure 5: FNA cell block, H & E, X 200
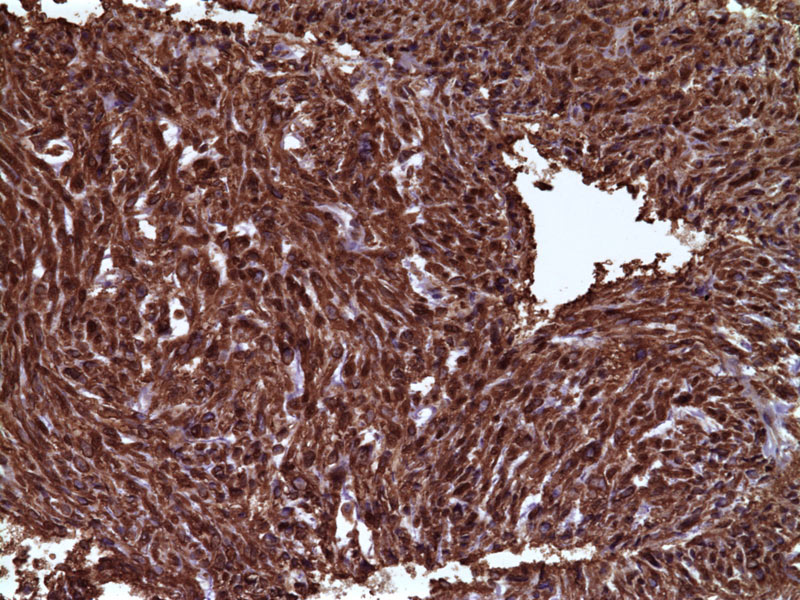
- Figure 6: FNA cell block, smooth muscle actin immunoperoxidase stain, X 200
Cytologic diagnosis: Leiomyosarcoma, low grade
Cytologic Findings:
- Tight clusters of spindled cells in parallel arrays
- Naked nuclei in background
- Granular eosinophilic cytoplasm
- Blunt-ended nuclei
- Occasional large pleomorphism nuclei
- Smooth muscle actin stain is positive
Discussion: Leiomyosarcoma (LMS) account for 5-10% of soft tissue sarcomas, and most occur in adults in the retro-peritoneum and axial soft tissue. Parenchymatous organs and bones are also rarely primary sites for this sarcoma. FNA of LMS can provide a pre-operative diagnosis in both primary and recurrent tumors.
Aspirates of low-grade classical LMS range from sparse to highly cellular and show cohesive, spindle-shaped cells aligned in parallel fascicles. Dispersed cells and stripped nuclei can also be seen, but the cohesive cells predominate. The cytoplasm is eosinophilic and granular. Nuclei are often blunt-ended (cigar-shaped), but may also be spindle-shaped or ovoid; nuclear segmentation or indentation is common in nuclei of both shapes. The nuclei contain evenly distributed chromatin, nucleoli, and occasional intranuclear inclusions can also be identified. Fibrotic connective tissue fragments may also be seen. High-grade classical LMS frequently shows background necrotic debris, anaplastic giant cells, coarse chromatin, and mitotic figures and lacks the cytoplasmic granularity and intranuclear inclusions seen in its low-grade counterpart.
Epithelioid LMS aspirates show a mixture of small and large spindled or round cells in parallel alignment. Myxoid LMS aspirates demonstrate abundant myxoid matrix containing large spindled and giant cells. Both Epithelioid and myxoid LMS lack the cytoplasmic granularity, intranuclear inclusions, and blunt-ended nuclei seen in low-grade classical LMS.
The differential diagnosis for LMS includes benign tumors, other soft tissue sarcomas, carcinoma, and melanoma. Aspirates of LMS can be differentiated from leiomyoma by the presence of closely packed cells which favors a malignant diagnosis. Necrosis, mitotic figures and cellular and nuclear pleomorphism are helpful, if present.
Wavy nuclei, as well as positive S-100 protein staining favor schwannomas and malignant peripheral nerve sheath tumors over LMS. Nodular fasciitis behaves distinctly from LMS, and smears of this tumor show ganglion-like plump histiocytes upon careful review. Aspirations of desmoid tumor, both intra and extra-abdominal, can be suggestive of LMS. However, the sparse to moderately cellular smears with bland, predominantly dissociated and slightly pleomorphism cells strongly suggest the diagnosis of desmoid tumor. Malignant fibrosis histiocytomas (MFH) can be differentiated from high grade LMS by the absence of smooth muscle marker positivity in MFH. Gastrointestinal stromal tumors can be differentiated by their positive staining for c-kit. Carcinomas and metastatic melanomas can be differentiated from LMS by their strong, diffuse staining for cytokeratin and S-100, HMB-45 or melan A, respectively.
LMS can be accurately diagnosed by FNA. Key features included the formation of fascicles with tightly grouped cells, blunt-ended nuclei with intranuclear inclusions, nuclear segmentation, and eosinophilic granular cytoplasm. Positive smooth muscle actin immunohistochemistry can be useful in differentiating this tumor from other malignanciesReferences:
- Klijanienko J, Caillaud J, Lagacé R, Vielh P. Fine-Needle Aspiration of Leiomyosarcoma: A Correlative Cytohistopathological Study of 96 Tumors in 68 Patients. Diag Cytopath 2003;28(3):119-25.
- Domanski HA, Åkerman M, Rissler P, Gustafson P. Fine-Needle Aspiration of Soft Tissue Leiomyosarcoma: An Analysis of the Most Common Cytologic Findings and the Value of Ancillary Techniques. Diag Cytopath 2006;34(9):597-604.
- Weiss SW, Goldblum J. Leiomyosarcoma. In:Weiss SW, Goldblum JR, editors. Enzinger and Weiss's Soft Tissue Tumors , 4 th ed. St. Louis : Mosby;2001. p.727-48.
Acknowledgement: Submitted by Aimee C. Popp, M.D. and Momin T. Siddiqui, M.D., FIAC. Emory University School of Medicine, Atlanta , GA