Case of the Month ...
Case History
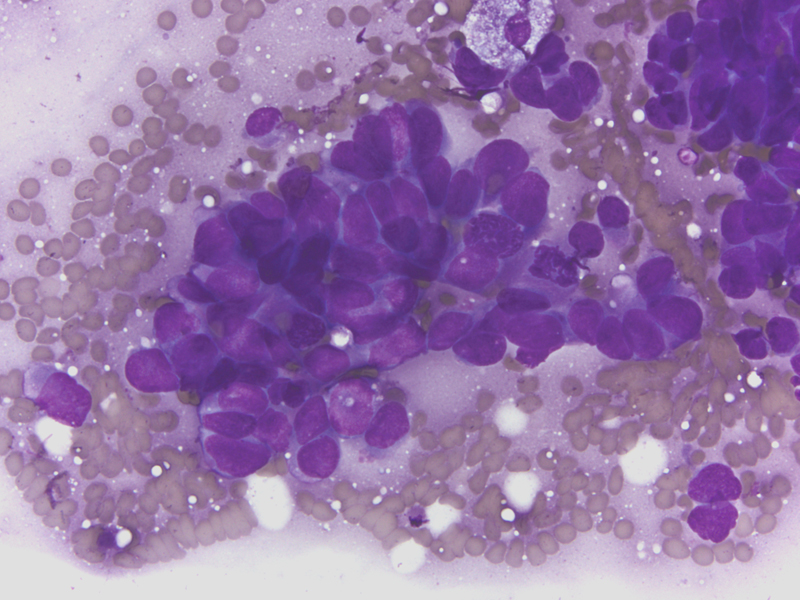
68-year-old man with 50 pack years of tobacco history presented with a 4 cm left lower lobe lung mass. CT-guided fine-needle aspiration performed.
Diagnosis & Discussion
click on image for larger version
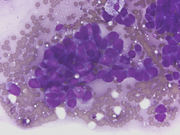
Figure 1
Image Figs:
- Figure 1: FNA cytology smear of lung mass, Diff-Quik stain, x600
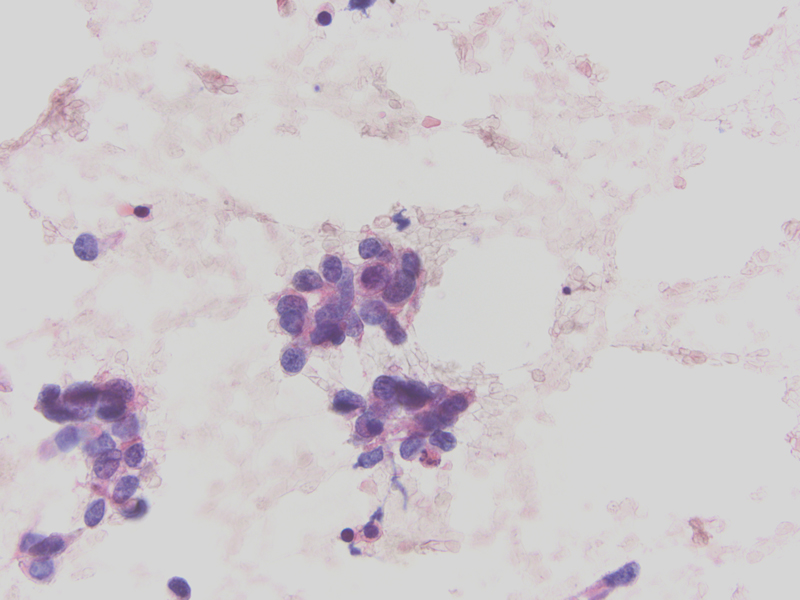
- Figure 2: FNA cytology smear of lung mass, Papanicolaou stain, x400
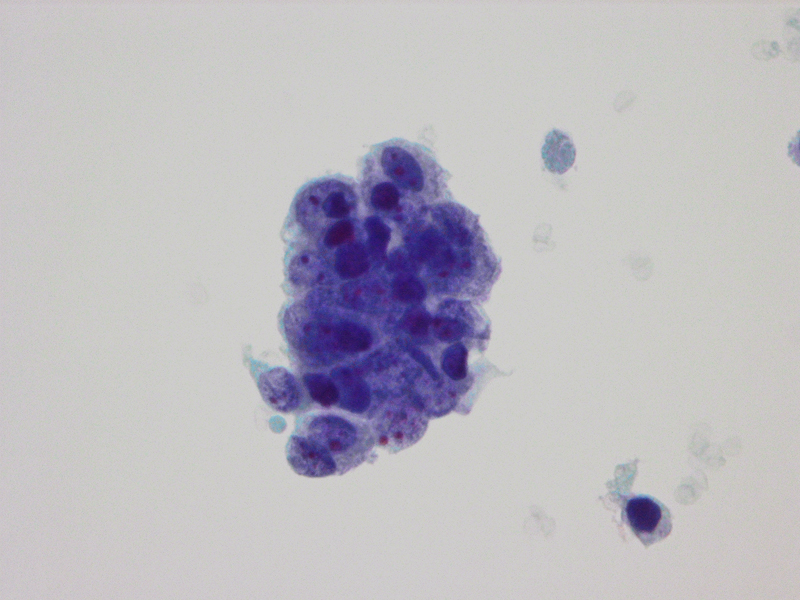
- Figure 3: FNA cytology ThinPrep of lung mass, Papanicolaou stain, x600
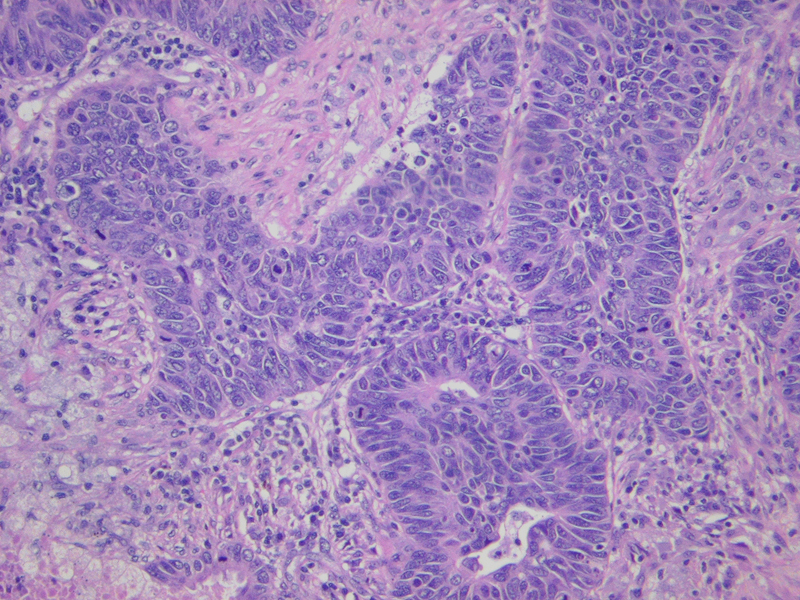
- Figure 4: Surgical resection of lung mass, H&E stain, x100
Questions:
- What is the diagnosis?
- Small cell carcinoma
- Large cell neuroendocrine carcinoma
- Large cell carcinoma
- Basaloid carcinoma
- Which of the following is characteristic of this entity and would be useful in distinguishing it from small cell carcinoma?
- A positive neuroendocrine immunostain
- Lack of nuclear molding
- Negative TTF-1 immunostain
- Negative p63 immunostain
- Features typical of this entity include all of the following except:
- Scant cytoplasm
- Large prominent nucleoli in most cells
- Hyperchromatic, granular chromatin
- Positive high molecular weight cytokeratin immunostain
- Which of the following immunostaining profiles would most support this diagnosis over small cell carcinoma and large cell neuroendocrine carcinoma?
- (+) chromogranin, (-) TTF-1, (-) p63, (+) PAX-5
- (+) chromogranin, (-) TTF-1, (+) HMWCK, (-) PAX-5
- (-) synaptophysin, (+) TTF-1, (-) HMWCK, (-) p63
- (+) synaptophysin, (+) TTF-1, (-) p63, (+) PAX-5
Discussion: Pulmonary basaloid carcinoma (BC) is an uncommon variant of large cell carcinoma with a poor prognosis that usually develops in males older than 60 years with a smoking history . It is defined as a variant of squamous cell carcinoma or large cell carcinoma depending on the presence or absence of squamous differentiation [basaloid squamous cell carcinoma (BSQCC) and BC, respectively]. [1-3] BC can show features similar to high-grade neuroendocrine carcinomas, including both small cell carcinoma (SCC) and large cell neuroendocrine carcinoma (LCNEC), in both cytological and histological specimens.
Cytomorphologic features of BC in fine-needle aspiration (FNA) include hyperchromatic nuclei with finely granular chromatin, nuclear molding, inconspicuous nucleoli, and scant cytoplasm, findings frequently observed in small cell carcinoma. [4,5] Cell arrangements include nests, sheets, and 3-dimensional clusters of basaloid cells in a necrotic background. [5,6] Larger cells showing moderate amount of cytoplasm, moderate pleomorphism, hyperchromasia, and occasional prominent nucleoli may be intermixed with the more typical small-to-medium sized cells. [6] The presence of squamous differentiation would support the diagnosis of BSQCC. Nuclear molding is both sensitive and specific in distinguishing SCC from non-small cell carcinoma, [7] but the presence of nuclear molding in cytologic specimens, particularly if it is focal, does not exclude the possibility of BC or BSQCC.
Histopathologic features of BC include lobular or anastomotic trabecular growth pattern with peripheral palisading, relatively small cuboidal-to-fusiform cells with hyperchromatic nuclei that lack prominent nucleoli, high mitotic rate, and necrosis, [2,3,8,9] SCC shows overlapping histologic features and may show nesting, trabeculae, peripheral palisading, rosette formation, or sheet-like growth. The tumor cells are usually <= the size of three small lymphocytes and have round, ovoid, or spindled nuclei and scant cytoplasm. Nuclear chromatin is granular and nucleoli are absent or inconspicuous. Nuclear molding is common. Mitotic rate is usually >60 mitoses per 2mm 2. [10] LCNEC may also show similar histologic features, including an organoid growth pattern with periperheral palisading, high mitotic rate, and necrosis, but the tumor cells are usually large, contain frequent and prominent nucleoli, and have moderate-to-abundant cytoplasm. [10] Confirmation of neuroendocrine differentiation in LCNEC is necessary using immunohistochemical markers. [10]
The immunohistochemical staining pattern of BC, as well as BSQCC, is distinct from both LCNEC and SCC. [2,11-19] High molecular weight cytokeratin (HMWCK) and p63 are positive in BC/BSQCC and negative in both LCNEC and SCC. [2,11-13] . Neuroendocrine markers, including synaptophysin and chromogranin, and TTF-1 are typically negative in BC and BSQCC, although they may display 1 or 2 neuroendocrine markers, as mentioned previously. [2,10,20] In contrast, neuroendocrine markers and TTF-1 are usually positive in both LCNEC and SCC. [2,10,20] PAX-5 immunohistochemical stain consistently shows strong positive nuclear staining in SCC and absence of nuclear staining in BC. [18] The immunopanel of HMWCK, TTF-1, p63, PAX -5, and more than one neuroendocrine marker would be helpful in distinguishing BC/BSQCC from SCC and LCNEC.
s described above, the overlap of cyto-histomorphologic features between BC/BSQCC and high-grade neuroendocrine carcinomas, particularly SCC, is considerable. Relying on morphologic features alone may result in the diagnosis of SCC and subsequent inappropriate therapy. Immunostains are very helpful in distinguishing these neoplasms.
Answers
- d
- c
- b
- b
REFERENCES
1. Kim DJ, Kim KD, Shin DH, Ro JY, Chung KY. Basaloid carcinoma of the lung: a really dismal histologic variant? Ann Thorac Surg 2003;76(6):1833-7.
2. Brambilla E, Travis WD, Colby TV, Corrin B, Shimosato Y. The new World Health Organization classification of lung tumours. Eur Respir J 2001;18(6):1059-68.
3. Brambilla E, Moro D, Veale D, Brichon PY, Stoebner P, Paramelle B, Brambilla C. Basal cell (basaloid) carcinoma of the lung: a new morphologic and phenotypic entity with separate prognostic significance. Hum Pathol 1992;23(9):993-1003.
4. Dugan JM. Cytologic diagnosis of basal cell (basaloid) carcinoma of the lung. A report of two cases. Acta Cytol 1995;39(3):539-42.
5. Ro YS, Park JH, Park CK, Lee CW. Basaloid carcinoma of the lung presenting concurrently with cutaneous metastasis. J Am Acad Dermatol 2003;49(3):523-6.
6. Khalbuss WE, Fischer G, Tutuncuoglu SO. Cytomorphology of basaloid (basal cell) carcinoma of the lung. Acta Cytol 2007;51(5):834-6.
7. Arora VK, Singh N, Chaturvedi S, Bhatia A. Significance of cytologic criteria in distinguishing small cell from non-small cell carcinoma of the lung. Acta Cytol 2003;47(2):216-20.
8. Moro D, Brichon PY, Brambilla E, Veale D, Labat F, Brambilla C. Basaloid bronchial carcinoma. A histologic group with a poor prognosis. Cancer 1994;73(11):2734-9.
9. Nagakawa H, Hiroshima K, Takiguchi Y, Yatomi M, Takahashi Y, Mikami M, Nakatani Y, Kuriyama T. Basaloid squamous-cell carcinoma of the lung in a young woman. Int J Clin Oncol 2006;11(1):66-8.
10. Travis WD, Brambilla E, Muller-Hermelink HK, Harris CC, editors. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon: IARC Press; 2004. 344 p.
11. Viberti L, Bongiovanni M, Croce S, Bussolati G. 34betaE12 Cytokeratin Immunodetection in the Differential Diagnosis of Small Cell Tumors of Lung. Int J Surg Pathol 2000;8(4):317-322.
12. Sturm N, Lantuejoul S, Laverriere MH, Papotti M, Brichon PY, Brambilla C, Brambilla E. Thyroid transcription factor 1 and cytokeratins 1, 5, 10, 14 (34betaE12) expression in basaloid and large-cell neuroendocrine carcinomas of the lung. Hum Pathol 2001;32(9):918-25.
13. Sturm N, Rossi G, Lantuejoul S, Laverriere MH, Papotti M, Brichon PY, Brambilla C, Brambilla E. 34BetaE12 expression along the whole spectrum of neuroendocrine proliferations of the lung, from neuroendocrine cell hyperplasia to small cell carcinoma. Histopathology 2003;42(2):156-66.
14. Pelosi G, Pasini F, Olsen Stenholm C, Pastorino U, Maisonneuve P, Sonzogni A, Maffini F, Pruneri G, Fraggetta F, Cavallon A and others. p63 immunoreactivity in lung cancer: yet another player in the development of squamous cell carcinomas? J Pathol 2002;198(1):100-9.
15. Wu M, Wang B, Gil J, Sabo E, Miller L, Gan L, Burstein DE. p63 and TTF-1 immunostaining. A useful marker panel for distinguishing small cell carcinoma of lung from poorly differentiated squamous cell carcinoma of lung. Am J Clin Pathol 2003;119(5):696-702.
16. Wu M, Szporn AH, Zhang D, Wasserman P, Gan L, Miller L, Burstein DE. Cytology applications of p63 and TTF-1 immunostaining in differential diagnosis of lung cancers. Diagn Cytopathol 2005;33(4):223-7.
17. Shtilbans V, Szporn AH, Wu M, Burstein DE. p63 immunostaining in destained bronchoscopic cytological specimens. Diagn Cytopathol 2005;32(4):198-203.
18. Sica G, Vazquez MF, Altorki N, Port J, Lee PC, Liu Y, Hyjek E, Saqi A. PAX-5 expression in pulmonary neuroendocrine neoplasms: its usefulness in surgical and fine-needle aspiration biopsy specimens. Am J Clin Pathol 2008;129(4):556-62.
19. Kargi A, Gurel D, Tuna B. The diagnostic value of TTF-1, CK 5/6, and p63 immunostaining in classification of lung carcinomas. Appl Immunohistochem Mol Morphol 2007;15(4):415-20.
20. Moro-Sibilot D, Lantuejoul S, Diab S, Moulai N, Aubert A, Timsit JF, Brambilla C, Brichon PY, Brambilla E. Lung carcinomas with a basaloid pattern: a study of 90 cases focusing on their poor prognosis. Eur Respir J 2008;31(4):854-9.
Case contributed by John P. Crapanzano, M.D.
Columbia Presbyterian Medical Center , New York , NY
PSC Case of the Month
December 2009