Case of the Month ...

Case History
A 64 year old postmenopausal female presented with a 1.5 cm mass in the upper, outer quadrant of her left breast. On mammography this was an isodense lobulated mass. Ultrasonography revealed a solid, hypoechoic complex cystic mass. The patient underwent a fine needle aspiration.
Diagnosis & Discussion
click on image for larger version
Figure 1
Image Figs:
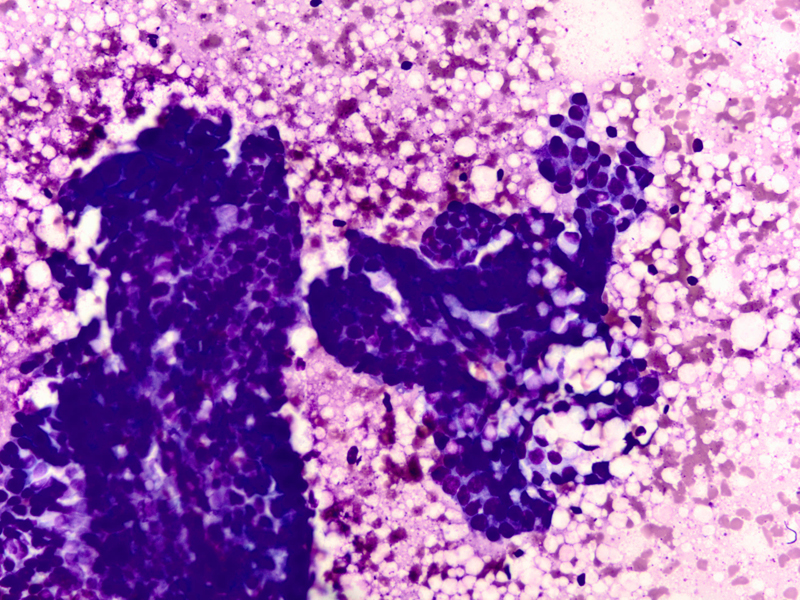
- Fig 1: FNA cytology, Diff-quik stain, X40
- Fig 2: FNA cytology, Diff-quik stain, X200
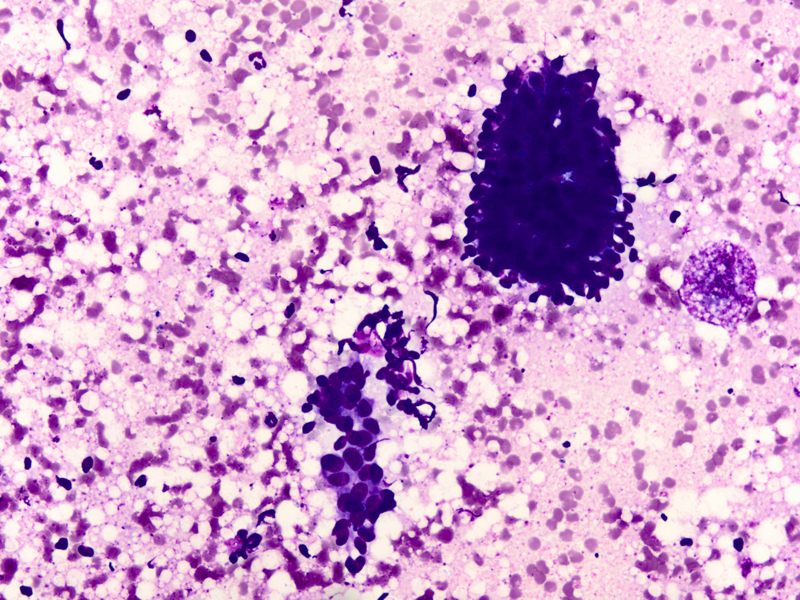
- Fig 3: FNA cytology, Diff-quik stain, X400
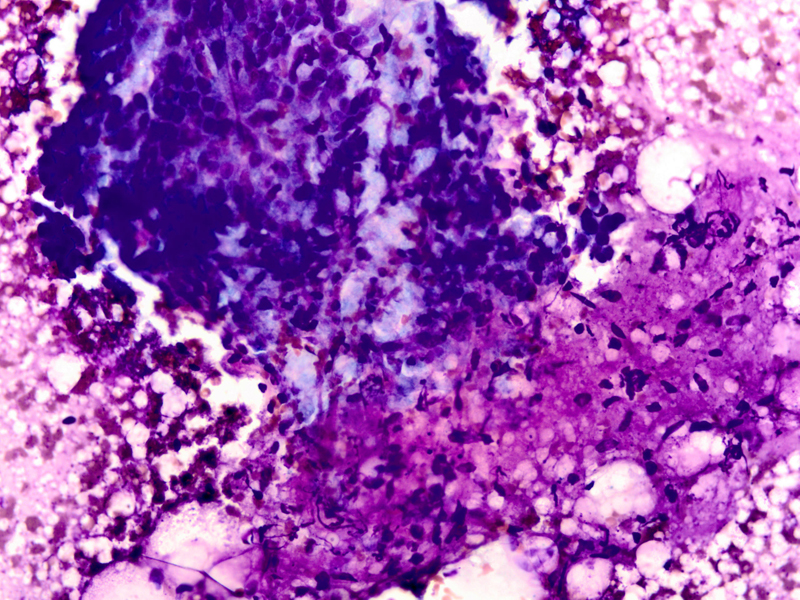
- Fig 4: FNA cytology, Diff-quik stain, X400
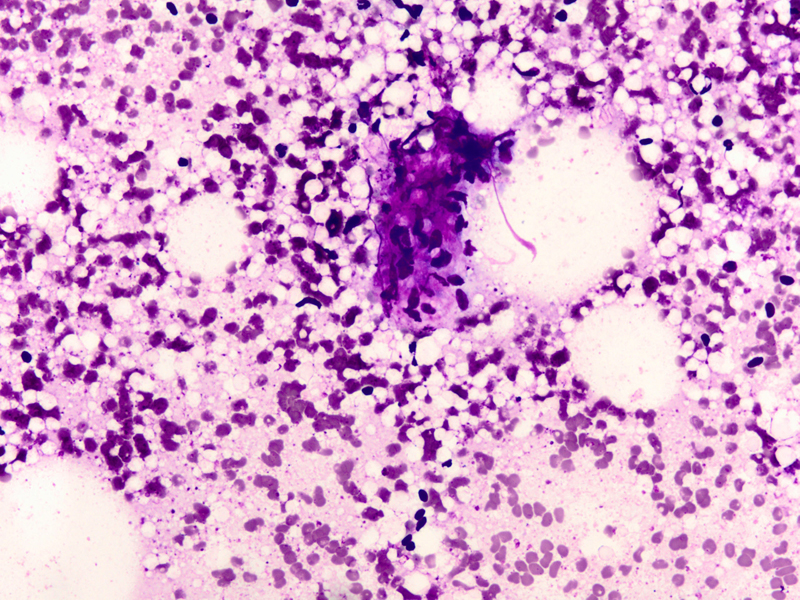
- Fig 5: FNA cytology, Diff-quik stain, X400
- Fig 6: FNA cytology, Diff-quik stain, X400
- Fig 7: FNA cytology, Diff-quik stain, X400
- Fig 8: Surgical resection, H and E stain, X100
- Fig 9: Surgical resection, H and E stain, X200
- Fig 10: Surgical resection, Smooth muscle actin, X200
Questions:
- What is the diagnosis?
- Adenomyoepithelioma
- Tubular carcinoma
- Phyllodes tumor
- Fibroadenoma
- What cytologic features are characteristic of this lesion?
- Branching clusters of ductal epithelial cells and myoepithelial cells, fragments of myxoid stroma and aggregates of spindled shaped myoepithelial cells
- Staghorn clusters, bare oval nuclei and fragments of fibromyxoid stroma
- Angulated epithelial cell clusters and an absence of bare oval nuclei
- Hypercellular stromal fragments and an absence of epithelial cell clusters
- What immunophenotype is characteristic of this lesion?
- Cytokeratin positive, calponin negative
- Cytokeratin positive, calponin positive
- EMA negative, cytokeratin negative
- S100 negative, smooth muscle actin negative
- Which of the following statements is true regarding this tumor?
- The majority are malignant
- Focal marked atypia may be seen, although the tumor is benign
- Distant metastasis is common
- Recurrences do not occur
Cytologic findings
- Moderately cellular smear
- Branching clusters of ductal epithelial cells, dissociated single cells, or rarely acinar or papillary arrangements
- Polygonal to round ductal epithelial cells with uniform nuclei, abundant cytoplasm and inconspicuous nucleoli
- Focal marked atypia may be seen in benign adenomyoepitheliomas (1).
- Abundant myoepithelial cells as round to spindled shaped cells, as bare oval nuclei in the background or overlying epithelial cell clusters, or as cells with clear cytoplasm
- Focal aggregates of spindled cells
- Fragments of myxoid or fibrous stroma
- Intranuclear inclusions (1) and intracytoplasmic vacuoles (2) have been described
- Thin proteinaceous debris, histiocytes and apocrine cells may be seen
Discussion: Adenomyoepithelioma was first reported by Hamperl in 1970 as an uncommon biphasic tumor composed of epithelial and myoepithelial cells (3). Adenomyoepitheliomas usually present as a single circumscribed mammary nodule. The fine needle aspiration findings in adenomyoepitheliomas have been described in only a few reports (1, 2, 4-11). It is important to recognize this entity as the radiologic and cytologic features can mimic malignancy. On cytology single enlarged atypical epithelial cells, presumed to be of myoepithelial origin due to staining with S-100 protein have been noted and led to the erroneous diagnosis of carcinoma (6). Only rarely can this diagnosis be made definitively on fine-needle aspiration biopsy (7). Histologic patterns include the tubular, lobulated and spindle cell variants (12). Biphasic pattern consists of tubules lined by cuboidal or columnar shaped epithelial cells surrounded by myoepithelial cell layer, Malignant adenomyoepitheliomas are usually characterized by cellular pleomorphism, necrosis, high mitotic activity and invasion of the surrounding tissue. Immunohistochemistry illustrates the biphasic nature of adenomyoepitheliomas with staining for low molecular weight cytokeratin and epithelial membrane antigen in the epithelial component and staining for smooth muscle actin, S-100 protein, calponin, p63 and maspin in the myoepithelial cell component (8)
The differential diagnosis on fine-needle aspiration includes
- Phyllodes tumors: epithelial and myoepithelial cells are seen; more numerous stromal cells and single spindled stromal cells (9, 10); single bare nuclei more elongated and abundant than in adenomyoepitheliomas (5).
- Myoepithelioma: prominent spindled cell component; lack epithelial component.
- Myofibroblastoma: neoplastic cells have longitudinal grooves (13).
- Fibroadenoma: can be confused with tubular variant of adenomyoepithelioma; staghorn epithelial groups and fibrillary (rather than dense stroma in adenomyoepithelioma) stroma (11).
- Tubular carcinoma: angular cell clusters and lack of myoepithelial cells Adenoid cystic carcinoma: biphasic pattern with three dimensional cribriform epithelial cell clusters and amorphous hyaline globules (9).
Treatment and prognosis
The majority of adenomyopeitheliomas are benign but local recurrences (12) and rarely distant metastases (14) have been described. The treatment for benign adenomyopithelioma is wide local excision.
References:
- Valente PT, Stuckey JH. Fine-needle aspiration cytology of mammary adenomyoepithelioma: report of a case with intranuclear cytoplasmic inclusions. Diagn Cytopathol 1994; 10:165-168.
- Iyengar P, Ali SZ, Brogi E. Fine needle aspiration cytology of mammary adenomyoepitheliom: a study of 12 patients. Cancer 2006; 108:250-6.
- Hamperl H. The myoepithelia (myoepithelial cells): Normal state; regressive changes; hyperplasia; tumors. Curr Top Pathol 1970; 53:161-220.
- Mercado CL, Toth HK, Axelrod D, Cangiarella J. Fine-needle aspiration biopsy of benign adenomyoepithelioma of the breast: radiologic and pathologic correlation in four cases. Diagn Cytopathol 2007;35:690-694.
- Birdsong GG, Bishara HM, Costa MJ. Adenomyoepithelioma of the breast: report of a case initially examined by fine-needle aspiration. Diagn Cytopathol 1993;9:547-550.
- Niemann TH, Benda JA, Cohen MB. Adenomyoepithelioma of the breast: fine-needle aspiration biopsy and histologic findings. Diagn Cytopathol 1995;12:245-250.
- Chang A, Bassett L, Bose S. Adenomyoepithelioma of the breast: a cytology dilemma. Report of a case and review of the literature. Diagn Cytopathol 2002; 26:191-196.
- Mathur SR, Karak K, Verma K. Adenomyoepithelioma of the breast: a potential diagnostic pitfall on fine needle aspiration cytology. Indian J Pathol Microbiol 2004;47:243-245.
- Ng WK. Adenomyoepithelioma of the breast: a review of three cases with reappraisal of the fine needle aspiration biopsy findings. Acta Cytol 2002;46:317-324.
- Kurashina M. Fine-needle aspiration cytology of benign and malignant adenomyoepithelioma: report of two cases. Diagn Cytopathol 2002;26:29-34.
- Viguer JM, Lopez-Ferrer P, Vicandi B et al. Cytologic features of the tubular variant of breast adenomyoepithelioma. Acta Cytol 2001;45:1090-1092.
- Tavassoli FA. Myoepithelial lesions of the breast: Myoepitheliosis, adenomyoepithelioma and myoepithelial carcinoma. Am J Surg Pathol 1991;15:554-568.
- Ordi J, Riverola A, Sole M et al. Fine needle aspiration biopsy of myofibroblastoma of the breast in a man: a report of two cases. Acta Cytol 1992;36:194-198.
- Loose JH, Patchefsky AS , Hollander IJ, Lavin LS, Cooper HS, Katz SM. Adenomyoepithelioma of the breast. A spectrum of biologic behavior. Am J Surg Pathol 1992;16:868-876.
Answers
- a
- a
- b
- b