Case of the Month ...
Case History
A 24 year-old female presented with two palpable masses in her right breast. On ultrasound, both masses were hypoechoic and lobulated. One measured 2.3 cm at the 2 o'clock position, 3 cm from the nipple and the other measured 0.8cm at the 7 o'clock position, 6 cm from the nipple. Ultrasound guided fine needle aspirations were performed on both masses. The patient also described two painful masses near the left scapula and in her left arm.
Diagnosis & Discussion
click on image for larger version
Image Figs:
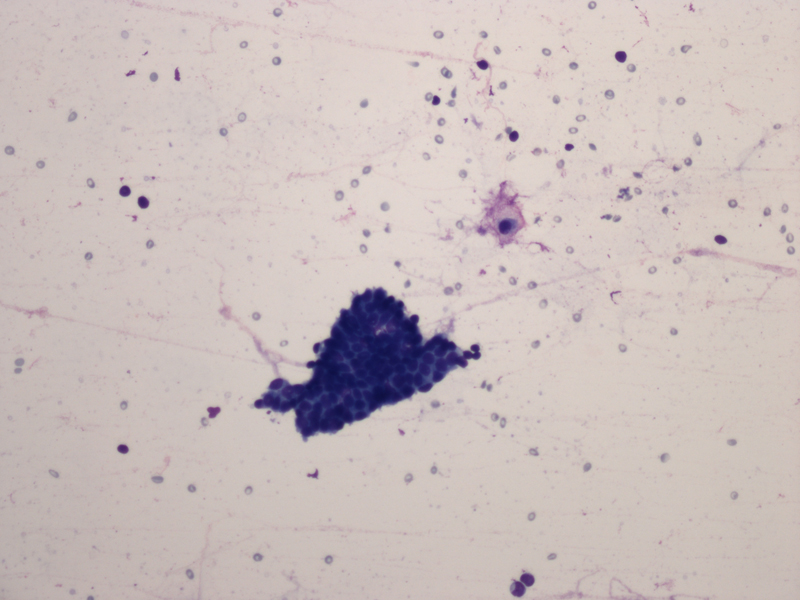
Figure 1. FNA cytology smear of breast mass, Diff-Quik stain, x20
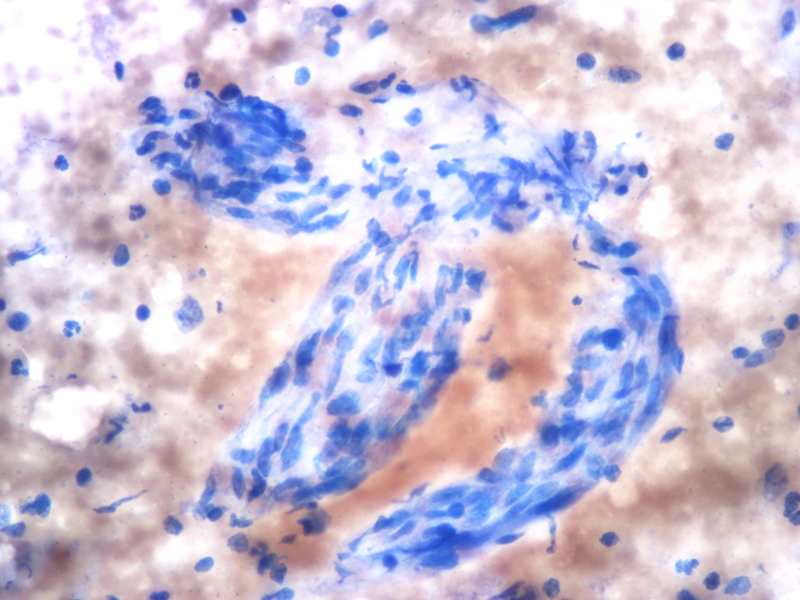
Figure 2. FNA cytology smear of breast mass, Diff-Quik stain, x20
Figure 3. FNA cytology smear of breast mass, Diff-Quik stain, x40
Questions:
What is the cytological diagnosis of her breast masses?
Fibroadenoma with myxoid changes
Phyllodes tumor
Neurofibroma
Fibromatosis
Nodular fascitis
What lesions would be included in the differential diagnosis?
Direct extension of dura-based tumor
Primary tumor of optic nerve sheath
Direct invasion of soft tissue-raised tumor
Metastatic tumor
Which of the following statements is true regarding this tumor?
Nodular fasciitis
Myofibroblastoma
Fibromatosis
Leiomyoma
Spindle cell lipoma
Phyllodes tumor
Metaplastic carcinoma
All of above
What immunostains are helpful in establishing the diagnosis?
Discussion:
vimentin
cytokeratin
S100
CD34
Beta-catenin
All of above
Neurofibromas are benign tumors of perineural cell origin that arise from elements of the peripheral nervous system (1). The majority of neurofibromas are often solitary lesions that occur in the dermis or subcutis. Neurofibromas in the skin are more common than those occurring in the deeper soft tissues. Neurofibroma of the breast is very rare (1-5). It is most commonly associated with neurofibromatosis Type 1 (NF1). The diagnosis of NF1 is based on clinical criteria established by the National Institutes of Health Consensus Development Conference (6). The most common clinical manifestations are six or more café au lait spots, two or more neurofibromas, two or more Lisch nodules, axillary or inguinal freckling, sphenoid wing dysplasia or thinning of a long bone cortex and optic glioma. Two or more of the criteria are required for diagnosis. Tumors occur in NF1 patients include neurofibroma, optic nerve glioma, leukemia, rhabdomyosarcoma, pheochromocytoma, and malignant peripheral nerve sheath tumor (7) (8). Our patient has a history of NF1. Her scapular mass and her left arm mass were associated with the left median nerve and on excision were Schwannomas. Sporadic cases of neurofibroma in the breast which are not related to NF1 are even rarer. When neurofibromas occur in the breast, they are most commonly associated with the nipple-areolar complex (1-5). In our case, the masses did not involve the nipple. These two masses showed similar cytologic features with spindled cells in a myxoid background (Figures 2 and 3). The nuclei of the spindled cells were wavy and slender. A few capillary vessels were seen associated with or detached from the myxoid stroma. Also, rare cohesive clusters of adjacent benign ductal epithelium with associated myoepithelial cells were noted (Figure 1).
Due to the presence of a myxoid background, one would consider common lesions in the breast such as fibroadenoma with myxoid changes, mucocele-like lesion, and mucinous adenocarcinoma in the differential diagnoses. However, neurofibromas in contrast to the other lesions mentioned does not have an epithelial component. One must be cautious as when benign ductal epithelial cells adjacent to a neurofibroma are aspirated, as were seen in our case, they may resemble the epithelial component of the other entities. The presence of spindled cells with wavy slender nuclei is a key, since it is not a feature of any of the above mentioned differential diagnoses. Myxomas should also be considered in differential diagnose but occur only rarely in the breast. They are less cellular than neurofibromas and the cells are small and stellate instead of elongated.
A number of spindle cell lesions should also be considered. The most important are cellular fibroadenomas, phyllodes tumors and low-grade fibromatosis like spindle cell carcinomas. Cellular fibroadenomas and benign phyllodes tumors show cellular stroma with bland spindled cells and benign ductal epithelial cells. The nuclei of the spindled cells are not wavy. When benign ductal cells adjacent to a neurofibroma are aspirated, they can be mistaken as the epithelial component of a cellular fibroadenoma or a benign phyllodes tumor. Also, not all neurofibromas show the characteristic wavy tapered nuclei. In difficult cases, an immunohistochemical stain for S-100 protein can be used to distinguish neurofibroma from the other entities. Low-grade fibromatosis like spindle cell carcinoma is a variant of metaplastic carcinoma with spindle cells of minimal cytological atypia. The presence of malignant epithelial cells and the lack of wavy nuclei of the spindled cells help to distinguish low-grade fibromatosis like spindle cell carcinoma from neurofibromas. Other differential diagnoses are less common, including fibromatosis, nodular fascitis, myofibroblastoma, inflammatory myofibroblastic tumor, leiomyoma and spindle cell lipoma. The presence of wavy tapered nuclei favors neurofibroma. Useful immunohistochemical markers include S100- protein for neurofibroma and beta-catenin, CD34, smooth muscle actin, and ALK.
Genetically, the NF1 gene is located in the pericentromeric region of the long arm of chromosome 17. Mutations in the NF1 gene lead to abnormal tumor suppression. NF1 also serves as a major risk factor in the development of several malignancies. There have been a few cases in the literature that show an increased risk of invasive ductal carcinomas of the breast in NF1 patients (3). The hypothesis for the association of these two conditions is that the NF1 gene and BRCA1 gene are located in close proximity on chromosome 17q. However, owing to the rarity of cases of concurrent NF1 and breast cancer, the statistical significance of the association of these two conditions can not be clearly established (9).Answers
- c
- h
- f
REFERENCES
Murat A, Kansiz F, Kabakus N, et al. Neurofibroma of the breast in a boy with neurofibromatosis type 1. Clin Imaging 2004; 28: 415-17.
Wakely PE Jr. Myxomatous soft tissue tumors. Correlation of cytopathology and histopathology. Ann Diagn Pathol 1999; 3: 227-42.
Millman SI, Mercado CL. An unusual presentation of neurofibromatosis of the breast. Breast J 2004; 10: 45-7.
Sherman JE, Smith JW. Neurofibromas of the breast and nipple areolar area. Ann Plast Surg 1981; 7: 302-7.
Fink D, Schneider C, Wight E, et al. Neurofibromatosis of the breast in a patient with Morbus von Recklinghausen. Gynakol Geburtshilfliche Rundsch 2000; 40: 47-9.
Gutmann DH, Aylsworth A, Carey JC, et al. The diagnostic evaluation and multidisciplinary management of neurofibromatosis 1 and neurofibromatosis 2. JAMA 1997; 278: 51-7.
Lin J, Martel W. Cross-sectional imaging of peripheral nerve sheath tumors: characteristic signs on CT, MR imaging, and sonography. AJR 2001; 176: 75-82.
Gokalp G, Hakyemez B, Kizildaya E, et al. Myxoid neurofibromas of the breast: mammographical, sonographical and MRI appearances. The British Journal of Radiology 2007; 80: 234-237.
The BT, Birrell G, Farrell A. Breast cancer in six women with neurofibromatosis type 1. The breast 1997; 6: 155-160.
Case contributed by
Xiasong Li, MD and Joan Cangiarella, MD.
Department of Pathology,
NYU School of Medicine, New York, NY