Case of the Month ...
Case History
A 41-year-old man presented with right upper quadrant pain, fever and an elevated white blood cell count. CT scan showed multiple ring enhancing lesions throughout the liver, a 3.5-cm mass in the tail of the pancreas, and lymphadenopathy in the portal, peripancreatic, and celiac axis. Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) biopsy of the pancreatic lesion was performed.
Diagnosis & Discussion
click on image for larger version
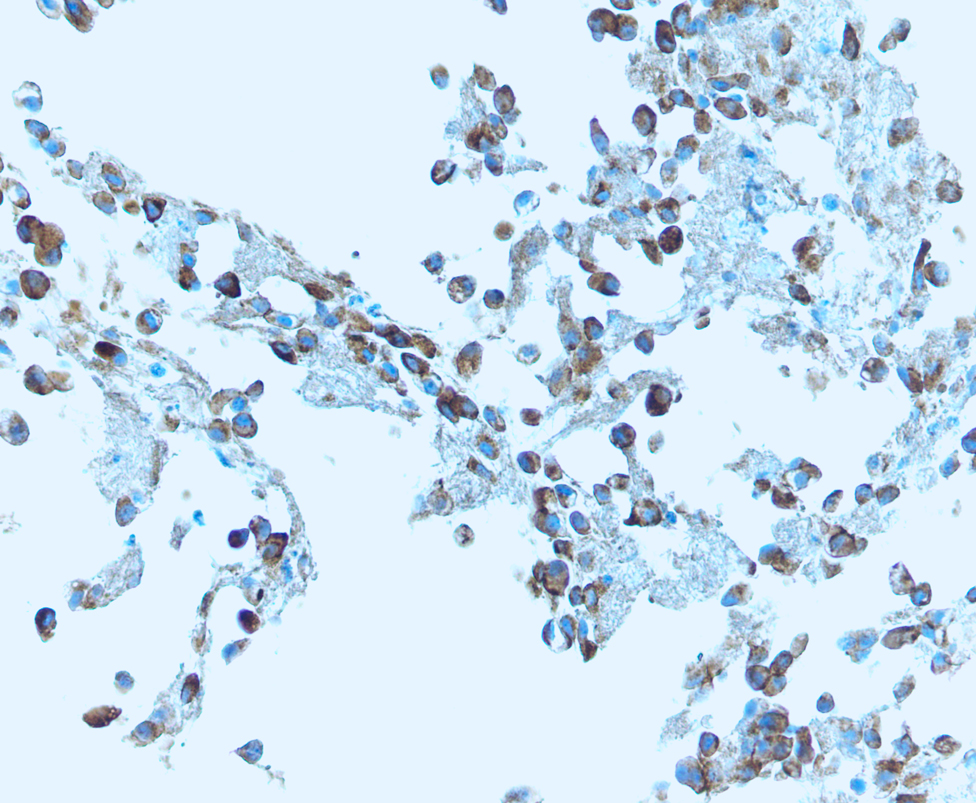
Image Figs:
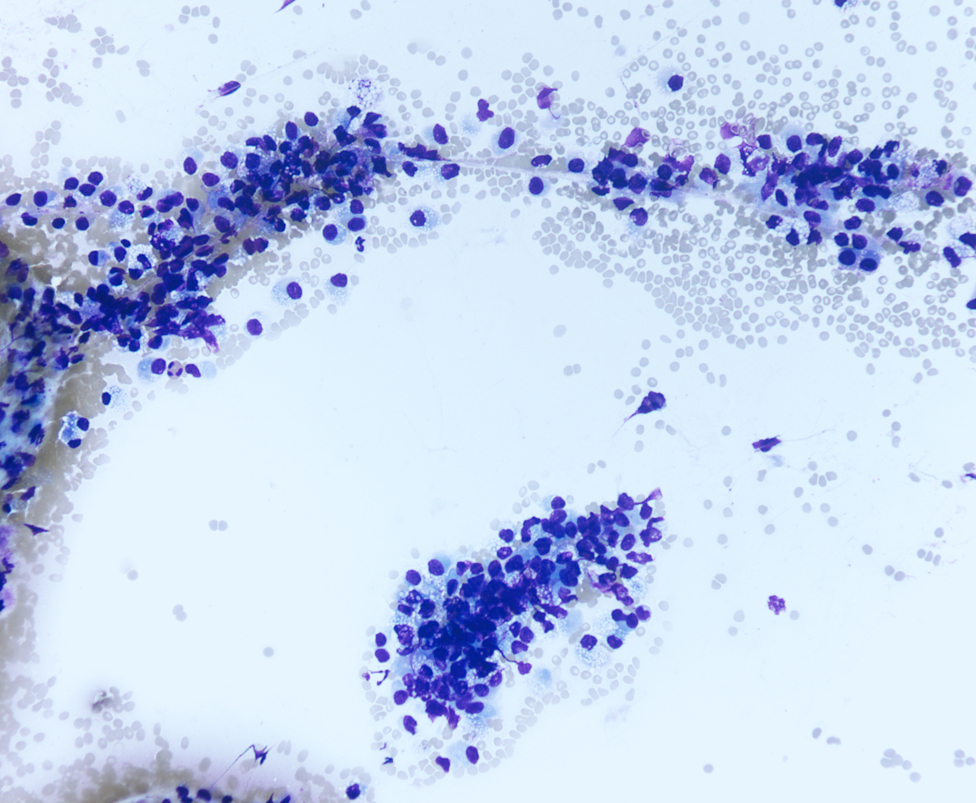
- Figure 1: FNA cytology, Diff-Quik stain, X100
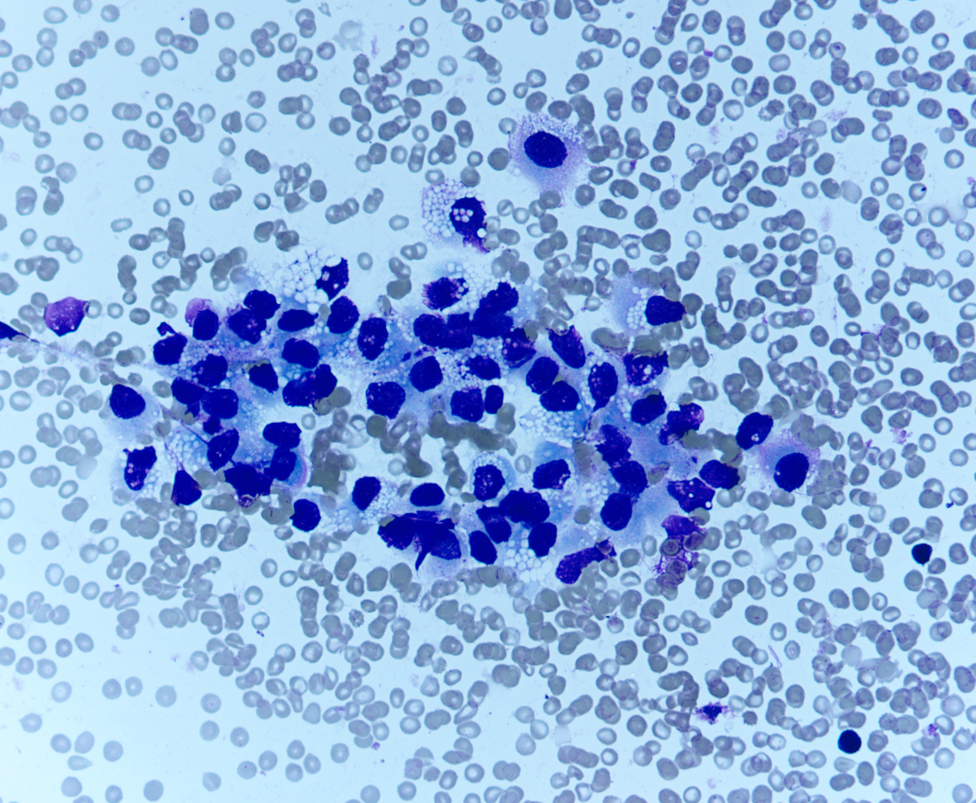
- Figure 2: FNA cytology, Diff-Quik stain, X400
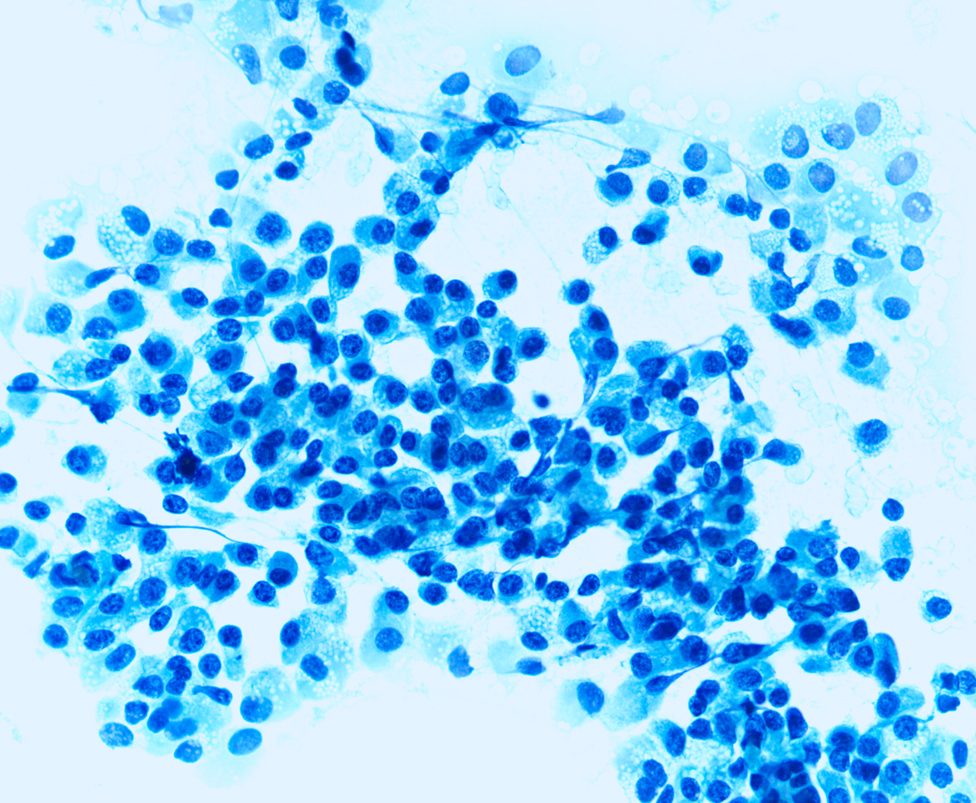
- Figure 3: FNA cytology, Papanicolaou stain, X400
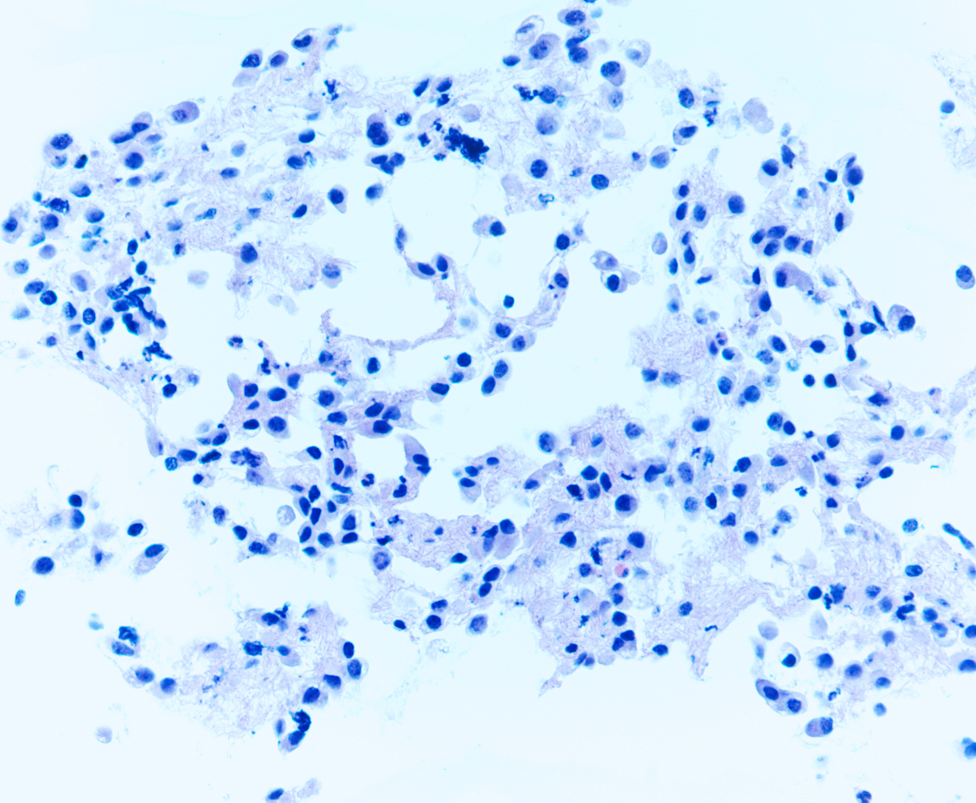
- Figure 4: FNA cytology, cell block, hematoxylin-eosin stain, X400
- Figure 5: FNA cytology, cell block, chromogranin immunoperoxidase stain, X400
- Figure 6: FNA cytology, cell block, synaptophysin immunoperoxidase stain, X400
Questions:
What is the diagnosis?
- Ductal adenocarcinoma
- Pancrreatic endocrine neoplasm
- Metastatic renal cell carcinoma
- Solid pseudopapillary tumor
- The cytoplasmic vacuoles seen on the aspirates of this tumor may be due to
- Lipid accumulation, oncocytic changes
- Clear cell changes, rhabdoid features
- Oncocytic changes, rhabdoid features
- Lipid accumulation, clear cell changes
- Which one of the followings is NOT the cytomorphologic features of this tumor?
- Large cytoplasmic vacuoles
- Polygonal or plasmacytoid cells
- Round or oval nuclei
- Stippled chromatin
- Which of the following statements is true regarding this tumor?
- Cytomorphologic analysis alone is sufficient for a diagnosis
- Non-immunoreactive with neuroendocrine markers
- Maybe associated with von-Hippel Lindau disease
- Always has a indolent clinical course
Discussion:
Pancreatic endocrine neoplasms (PENs) are relatively uncommon lesions, accounting for 1-2% of all pancreatic neoplasms. 1 Since the advent of endoscopic ultrasound (EUS), lesions of the pancreas can be better visualized and appropriately sampled with fine-needle aspiration (FNA) biopsy. In most cases, diagnosis of PENs can be rendered without difficulty based on cytomorphologic and immunophenotypic features. 2-6 The classical cytomorphologic features of PENs include single to loosely cohesive monotonous polygonal cells with finely granular cytoplasm and stippled (salt and pepper) chromatin. The nuclei are eccentrically located, giving a plasmacytoid appearance. However, uncommon cytomorphologic features may impose a diagnostic challenge. Within the cytoplasm, oncocytic changes, rhabdoid features, clear cells and lipid-rich variant have been documented in the literature of surgical pathology. 7-11 Recently there are two case reports demonstrating prominnet cytoplasmic vacuoles in PENs with one being clear cell variant and the other being lipid-rich variant. 12,13 The cytoplasmic vacuoles seen in PENs are often fine or small, in contrast to large vacuoles that might be seen in solid pseudopapillary neoplasm of the pancreas. 14 These cytoplasmic vacuoles are best appreciated on the slides stained with Diff-Quik technique. The presence of prominent cytoplasmic vacuoles significantly expends the differential diagnosis, including ductal adenocarcinoma, acinar cell carcinoma, solid pseudopapillary tumor, metastatic adrenocortical carcinoma and renal cell carcinoma. Positive immunostains with neuroendocrine markers such as chromogranin and synaptophysin help establish the diagnosis of PENs with this uncommon cytomorphologic feature.
The nature of cytoplasmic vacuoles seen in pENs is uncertain. These vacuoles may be caused by accumulation of glycogen, mucin, or lipid in the cytoplasm or just vacuolar degenerative changes. 10,11,15 Distinction of clear cell and lipid-rich variants may have clinical implications because they differ in their clinicopathologic characteristics. Unlike the clear cell variant, the lipid-rich counterpart most likely has no association with von Hippel-Lindau disease. 10,11 However, it is very difficult, if not impossible, to separate these two variants based on the cytomorphologic evaluation alone. Clinical-pathological correlation is crucial to exclude potential association with von Hippel-Lindau disease. PENs are well known to have variable biologic behaviors. Since there are only a very limited number of cases being reported, potential prognostic value of this morphologic variant is unknown.Answers
- b
- d
- a
- c
REFERENCES
Heitz PU, Komminoth P, Perren A, Klinstra DS, Dayal Y, Bordi C, Lechago J, Centeno BA, Kloppel G. Tumours of the endocrine pancreas. In: DeLellis RA, Lloyd RV, Heitz PU, Eng C, editors. World Health Organization Classification of Tumours Pathology & Genetics of Tumours of Endocrine Organs. Lyon, France: IARC Press. 2004; p175-208.
Collins BT, Cramer HM. Fine-needle aspiration cytology of islet cell tumors. Diagn Cytopathol 1996; 15:37-45.
Gu M, Ghafari S, Lin F, Ramzy I. Cytologic diagnosis of endocrine tumors of the pancreas by endoscopic ultrasound-guided fine-needle aspiration biopsy. Diagn Cytopathol 2004; 32:204-210.
Jimenez-Heffernan JA, Vicandi B, Lopez-Ferrer P, Gonzalez-Peramato P, Perez-Campos A, Viguer JM. Fine needle aspiration cytology of endocrine neoplasms of the pancreas. Morphologic and immunocytochemical findings in 20 cases. Acta Cytol. 2004; 48:295-301.
Chatzipantelis P, Salla C, Konstantinou P, Karpumpalis I, Sakellariou S, Doumani I. Endoscopic Ultrasound-guided Fine-Needle Aspiration Cyology of Pancreatic Neuroendocrine Tumors. Cancer Cytopathol 2008; 114:255-262.
Figueiredo FA, Giovannini M, Monges G, Charfi S, Bories E, Pesenti C, Caillol F, Delpero JR. Pancreatic endocrine tumors: a large single-center experience. Pancreas 2009; 38:936-940.
Perez-Montiel MD, Frankel WL, Suster S. Neuroendocrine carcinomas of the pancreas with 'Rhabdoid' features. Am J Surg Pathol 2003; 27:642-649.
Serra S, Asa SL, Chetty R. Intracytoplasmic inclusions (including the so-called rhabdoid phenotype) in pancreatic endocrine tumors. Endocrine Pathol 2006; 17:75-81.
Radi MJ, Fenoglio-Preiser CM, Chiffelle T. Functioning oncocytic islet-cell carcinoma. Report of a case with electron-microscopic and immunohistochemical confirmation. Am J Surg Pathol 1985; 9:517-524.
Hoang MP, Hruban RH, Albores-Saavedra J. Clear cell endocrine pancreatic tumor mimicking renal cell carcinoma. Am J Surg Pathol 2001; 25:602-609.
Singh R, Basturk O, Klimstra DS, Zamboni G, Chetty R, Hussain S, La Rosa S, Yilmaz A, Capelli P, Capella C, Cheng JD, Adsay NV. Lipid-rich variant of pancreatic endocrine neoplasms. Am J Surg Pathol 2006; 30:194-200.
Safo AO, Li RW, Vickers SM, Schmechel SC, Pambuccian SE. Endoscopic ultrasound-guided fine-needle aspiration diagnosis of clear-cell pancreatic endocrine neoplasm in a patient with von Hippel-Lindau disease: a case report. Diagn Cytopathol 2009; 37:365-372.
Ayub SB, Dodge J. Lipid-rich variant of pancreatic endocrine neoplasms: a case report. Acta Cytol 2010; 54 (5 Suppl):829-834.
Jhala N, Siegal GP, Jhala D. Large, clear cytoplasmic vacuolation: an under-recognized cytologic clue to distinguish solid pseudopapillary neoplasms of the pancreas from pancreatic endocrine neoplasms on fine-needle aspiration. Cancer Cytopathol 2008; 114:249-254.
Frankel WL. Update on pancreatic endocrine tumors. Arch Pathol Lab Med 2006; 130:963-966.
Case contributed by
Contributed by Gillian H. Levy, MD and Guoping Cai, MD
Department of Pathology
Yale University School of Medicine