Case of the Month ...
Clinical History:
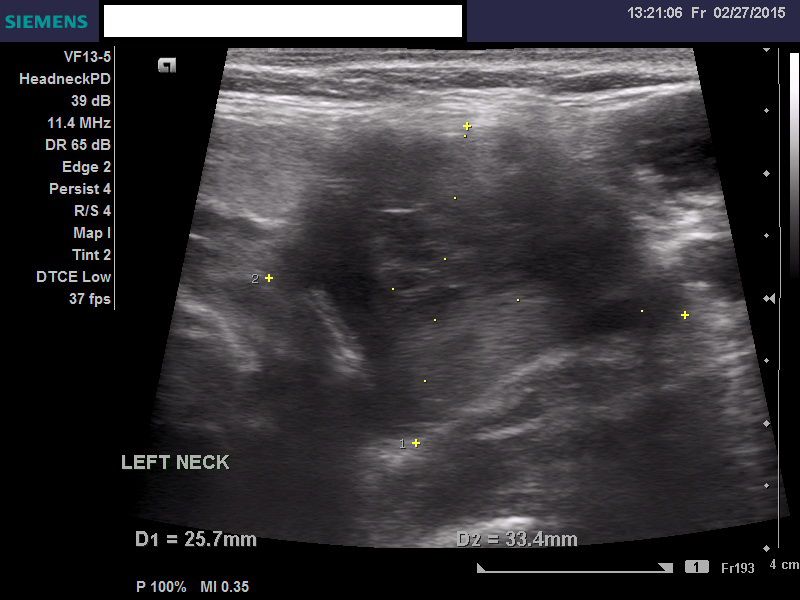
A 57-year-old woman presented with a left upper neck mass enlarging over the last three (3) years, non-tender to palpation. Ultrasound guided fine needle aspiration biopsy was performed. Subsequent imaging showed a 4.1 cm heterogeneous mass splaying the left carotid bifurcation, with internal flow voids. An excision was performed several weeks later.
Diagnosis & Discussion
click on image for larger version
Images 1-7:
Figure 1: Ultrasound Image
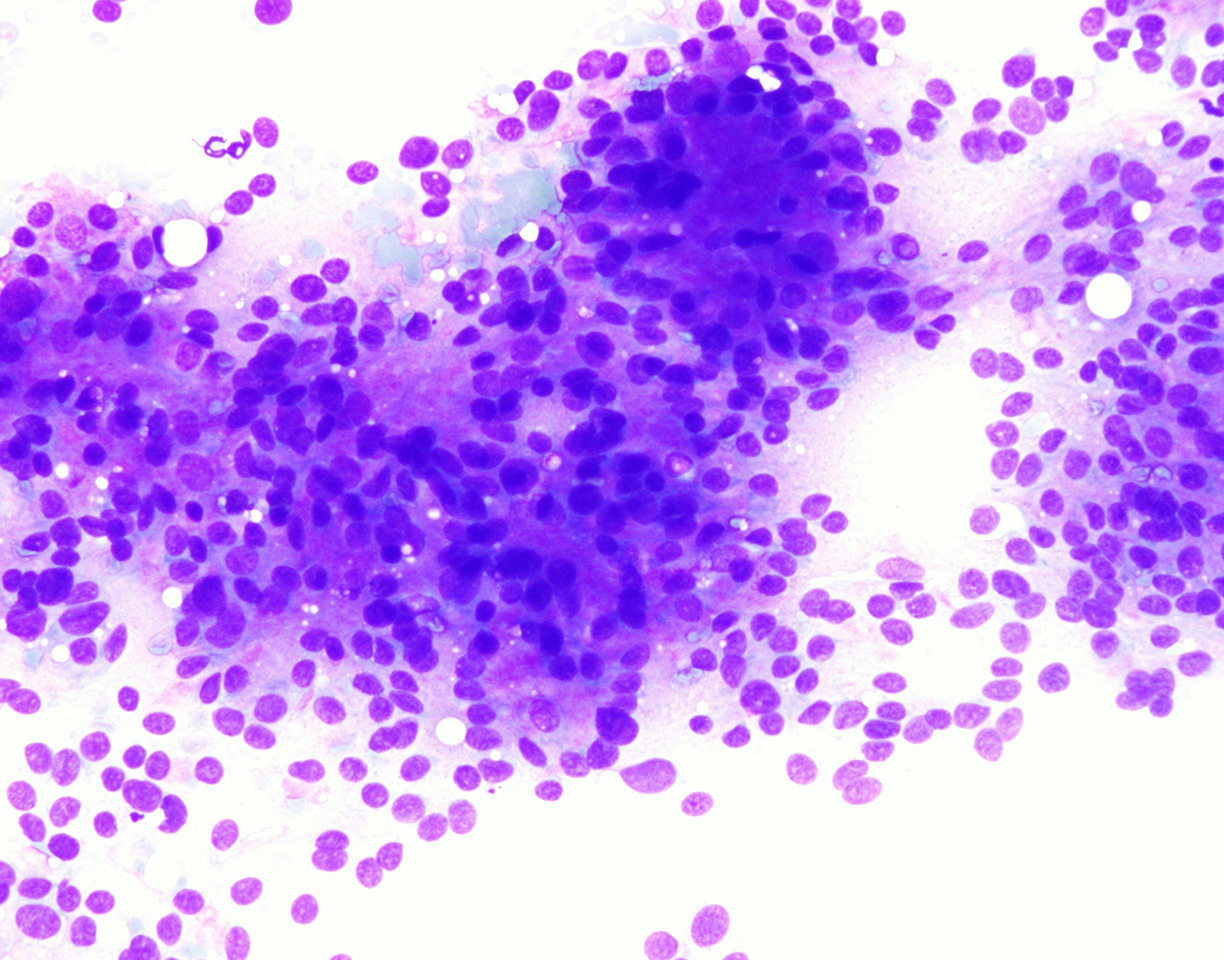
Figure 2: FNA Cytology, Diff-Quik, x100
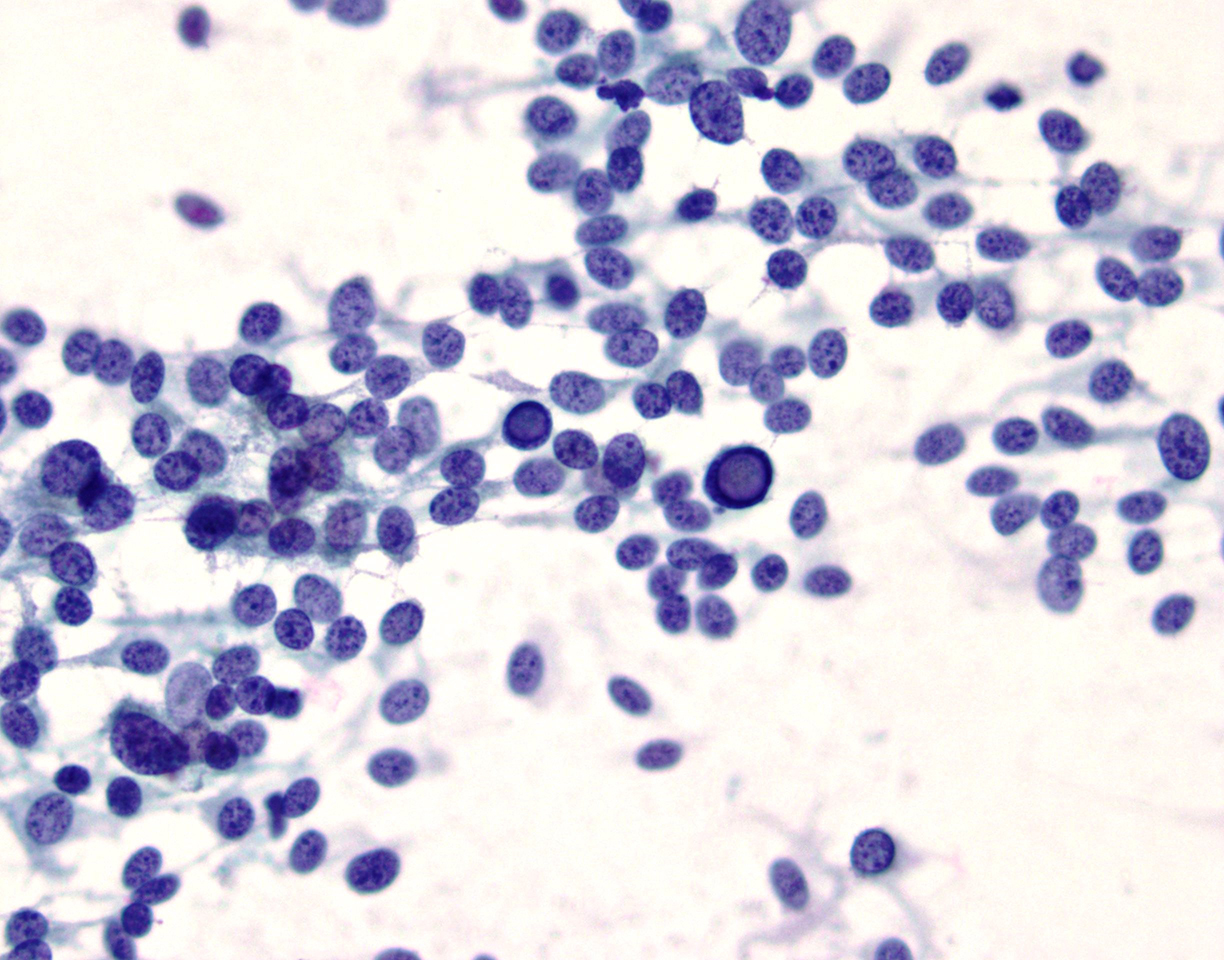
Figure 3: FNA Cytology, Diff-Quik, x200
Figure 4: FNA Cytology, Pap, x400
Figure 5: MRI Image
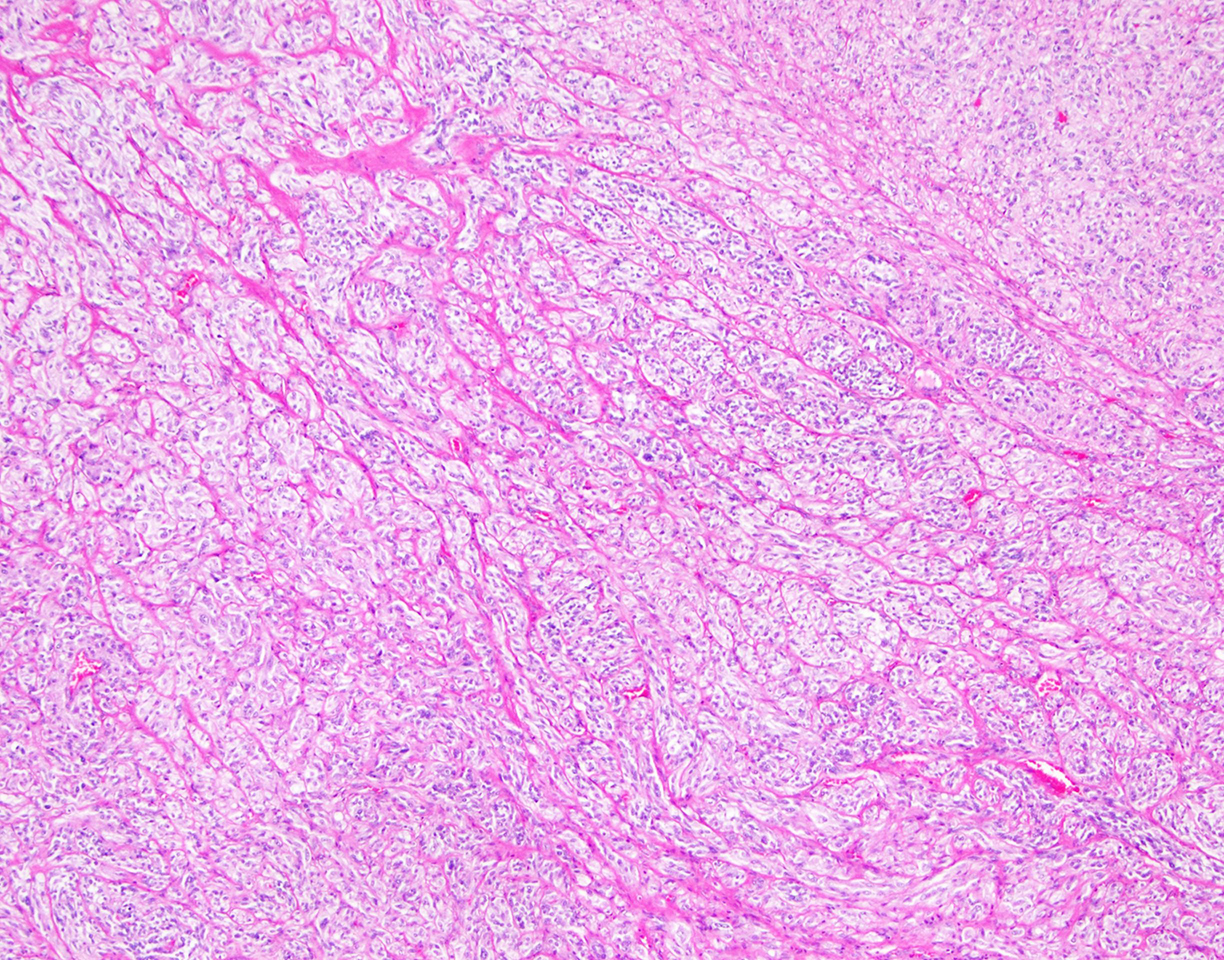
Figure 6: Surgical Resection, H&E, x40
Questions:
- Based on clinical history, location, imaging, cytological and histologic features, which of the following is the most appropriate diagnosis?
- Medullary thyroid carcinoma
- Melanoma
- Paraganglioma
- Pleomorphic lipoma
- Which immunostain panel would be most helpful to confirm this diagnosis?
- Synaptophysin, Chromogranin, Ki67
- HMB45, Melan-A, SOX-10
- S100, CAM5.2, CD34
- TTF-1, calcitonin, PAX8
- Which features could indicate malignancy/metastasis potential in a carotid body tumor?
- Necrosis
- Vascular invasion
- Atypical mitotic figures
- All of the above
- Which immunostain would be most useful to distinguish paraganglioma from a neuroendocrine tumor?
- Synaptophysin
- CAM5.2
- TTF-1
- Calretinin
Discussion:
The smears in this case show ovoid and spindle cells arranged in loosely cohesive groups and clusters. The chromatin of the cells is fine and granular with scattered intranuclear inclusions. Taking the clinical history and location into account, a diagnosis of findings suggestive of a carotid body tumor (paraganglioma) was rendered. Subsequent imaging showed a 4.1 cm heterogeneous mass splaying the left carotid bifurcation, with internal flow voids on MRI. Several weeks later surgical resection was performed, where Immunohistochemical confirmatory stains showed tumor cells positive for chromogranin, synaptophysin, and S-100. Ki67 labeling showed a mitotic index ranging from 5-10% in varying areas of the tumor. These findings confirmed the diagnosis of paraganglioma.
A carotid body tumor, also called a chemodectoma, is a rare neoplasm of the oxygen-sensing chemoreceptor organ located at the posterior aspect of the common carotid bifurcation. This chemoreceptor organ is involved in control of respiration, blood pressure, and heart rate. The head and neck in general are the most common anatomic sites for extra-adrenal paragangliomas, with carotid body, middle ear and vagus nerve as the most common subsites. There is a predilection for head and neck paragangliomas in women and within the 5thto 6th decades. Men tend to be more affected when it associated with an inherited or familial tumor. Patients present with a slow growing painless mass, maybe pulsatile, and may have related symptoms depending on location in the head and neck region. The majority of these tumors are benign, although malignancy has been reported and suggested features include central necrosis, vascular invasion and presence of atypical mitotic figures.
There is debate over fine needle aspiration of paragangliomas in the head and neck region regarding negative side effects. These include the possibility of hemorrhage, vasovagal reaction, or hypertensive crisis due to secretion of norepinephrine, although many biopsies have been performed without complication, especially when the diagnosis of paraganglioma is not in the differential and unsuspected. One case of cerebral artery thromboembolism has been reported. Additional studies to help confirm the cytologic diagnosis include ultrasound with color Doppler, computed tomography (CT) scan, magnetic resonance imaging (MRI), or carotid angiogram. Sampling, if performed, is recommended to be done using ultrasound guidance to minimize risk of penetrating the vessel wall.
The cells of a carotid body tumor/paraganglioma include chief cells and sustentacular cells. The chief cells are the main cell type (type I cells) and are of neuroectodermal origin. The sustentacular cells (type II cells) are the supporting cells in the stroma surrounding the chief cells. The typical cytologic features include abundant cytoplasm, spindle-shaped cells, and indistinct cytoplasmic outlines and granulations. In aspiration specimens, the smears may be bloody and dilute the cells, which may be singly or in small groups with an acinar pattern. There tends to be lack of necrosis or mitotic figures, and multinucleated and giant cells have been reported. The chief cells are highlighted by neuroendocrine markers including synaptophysin, chromogranin, and CD56, while the sustentacular cells are highlighted uniformly with S-100 immunostain.
The main differential diagnosis for a carotid body tumor presenting as a neck mass include a thyroid neoplasm, enlarged lymph node, branchial cleft cyst, parotid gland/salivary neoplasm, neurofibroma, or carotid artery aneurysm. Based on the cytomorphology, important considerations include other neuroendocrine tumors such as medullary carcinoma of the thyroid, neuroendocrine carcinoma, and hyalinizing trabecular tumor of the thyroid; keratins would be useful to aid in this distinction, being negative in paragangliomas and positive in neuroendocrine tumors.
Answers:
1. C
2. A
3. D
4. BReferences:
Chand P, Singh R, Singh B, Singla RL. Carotid Body Tumor Presenting as Parotid Swelling Misdiagnosed as Pleomorphic Adenoma: A Rare Presentation. Niger J Surg. 2015 Jul-Dec; 21(2): 157-158.
Das DK, Gupta AJ, Chowdhury V, et al. Fine-Needle Aspiration Diagnosis of Carotid Body Tumor: Report of a Case and Review of Experience with Cytologic Features in Four Cases. Diagn Cytopathol. 1996; 17(2): 143-147.
Dundas KE, Wong MP, Suen KC. Two Unusual Benign Lesions of the Neck Masquerading as Malignancy on Fine-Needle Aspiration Cytology. Diagn Cytopathol. 1995; 12(3): 272-278.
Hunt, JL. Diseases of the Paraganglia System. In: Head and Neck Pathology. Thompson LDR, ed. Philadelphia, Pennsylvania: Saunders; 2014: 668-678.
Jashnani KD, Patil RD, Balsarkar DJ. Loose cell clusters with vascular coats: Zellballen pattern of paraganglioma on cytology. J Cytol. 2013 Oct-Dec; 30(4): 278-279.
Naniwadekar MR, Jagtap SV, Kshirsagar AY, Shingagare SA, Tata HR, Sahoo K. Fine Needle Aspiration Diagnosis of Carotid Body Tumor in a Case of Multiple Paragangliomas Presenting with Facial Palsy: A Case Report. Acta Cytologica. 2010 July-Aug; 54(4): 635-639.
Contributed by:
Jeanine Chiaffarano DO