Case of the Month ...
Clinical History:
A 42 year old female with no significant past medical history was found to have a 2.6 cm thyroid nodule at right lower lobe. An ultrasound guided fine-needle aspiration biopsy was performed.
Diagnosis & Discussion
click on image for larger version
Figure 4 Figure 5 Figure 6 Images 1-6:
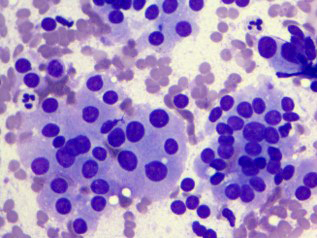
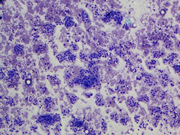
Figure 1: Thyroid FNA, Diff-quik Stains, 100 X.
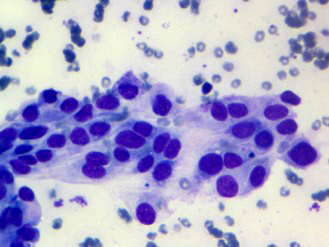
Figure 2: Thyroid FNA, Diff-quik Stains, 400 X.
Figure 3: Thyroid FNA, Diff-quik Stains, 400 X.
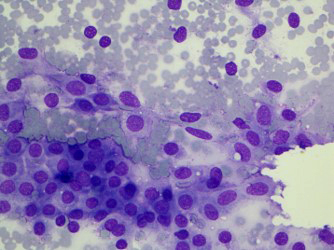
Figure 4: Thyroid FNA, Diff-quik Stains, 400 X.
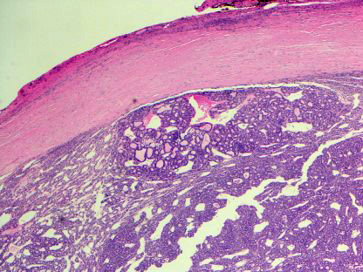
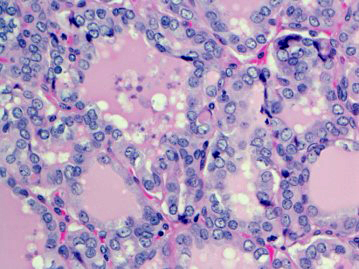
Figure 5: Thyroid surgical resection, H&E Stain, 40X.
Figure 6: Thyroid surgical resection, H&E Stain, 200X.
Figure 1: Show low power view of cellular smear in small groups or microfollicles.
Figure 2-4: Show high power view in Diff-quik, Figure 4 can appreciate nuclear feature better due to light hematoxylin stain.
Figure 5: Resection, lower power view, encapsulated.
Figure 6: Resection, high power view, nuclear feature.
Questions:
- Based on clinical history, cytological and surgical features, which of the following is the most appropriate diagnosis?
- Benign follicular nodule
- Follicular adenoma
- Medullary carcinoma
- NIFTP
- Papillary carcinoma
- Which cytology feature would be most unique in this entity?
- Dense colloid and large sheets of cells
- Cellular smear with microfollicles pattern without nuclear atypia
- Abundant small clusters with moderate nuclear atypia
- Marked nuclear atypia with nuclear inclusions
- Which is the next step would be most helpful to confirm the diagnosis presurgically?
- Immunostain HBME1, CK19
- Calcitonin, CEA, Congo red
- Collect tissue for cytogenetics
- Synaptophysin, Chromogranin, Ki67
- Do nothing.
- What kind of genetic change would be common in this entity?
- RET mutation
- RET-PTC rearrangement
- BRAF V600E mutation
- TERT promoter mutation
- RAS family mutation
Discussion:
The noninvasive encapsulated follicular variant of papillary thyroid carcinoma (EFVPTC) was recently renamed as noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) due to its unique behavior and good prognosis1. NIFTP behaves in an indolent manner with a much lower frequency of extrathyroid extension, positive margins, nodal metastases and recurrence2. Castro et al. reported that this tumor has PAX8-PPAR rearrangements and RAS mutations similar to the follicular adenoma/carcinoma3. Rivera et al, reported the K601E and G474R BRAF mutations in this tumor were different from V600E of classic papillary thyroid carcinoma4. The treatment for NIFTP is different from traditional treatment for papillary thyroid carcinoma. Conservative surgery such as lobectomy instead of total thyroidectomy is recommended for this entity1.
Although histologic criteria have been devised and recommended by a panel of experts5, diagnosing this tumor pre-surgically by fine needle aspiration (FNA) is still a challenge. There are some reports describing the cytologic features of NIFTP, especially in recent years. Three cases of NIFTP were reported as benign on FNA diagnosis in Turkey6. Yang7 compared 72 cases of NIFTP to 37 cases of encapsulated FVPTC with invasion (IEFVPTC) and reported hypercellularity in 5.6% of NIFTP cases vs. 8.1% in IEFVPTC cases; diffuse papillary thyroid carcinoma (PTC) nuclear features present in 44% of NIFTP and 45.9% of IEFVPTC. Strickland8 reported NIFTP is distinct from benign nodules due to nuclear atypia that is more significant than atypia of undetermined significant using nuclear atypical score criteria which include nuclear atypia using three parameters: nuclear size/shape, nuclear membrane and chromatin. Jaconi reported NIFTP was mostly diagnosed as Bethesda thyroid categories III/IV and there were overlapping features between NIFTP and FVPTC and benign nodules in 200 cases 9. Chandler reported NIFTP can be differentiated from invasive or infiltrative FVPTC by the presence of microfollicular pattern and absence of nuclear pseudo inclusions10. Brandler studied 56 NIFTP, 67 classic PTC, and 30 follicular adenoma (FA) cases and concluded cytomorphological features and surgical diagnosis of those cases may be used as clues to distinguish them on FNA aspiration11. Bizzarro found the majority of NIFTPs can be discriminated from IFVPTC by cytomorphology12. Singh found among 174 patients with surgery for PTC, only 21 patients were diagnosed with NIFTP postoperatively, and were less likely to have a preoperative malignant cytological diagnosis for NIFTP than classic PTC13. However, Zhao’s work on 50 NIFTP and 47 IFVPTC cases conclude it is unlikely to distinguish most cases using FNAB14 From the reports cited, it is clear that NIFTP diagnosis by FNA is a challenge due to its nature of a low-grade neoplasm. However, accurate diagnosis pre-surgically is critical for clinician and patient to prepare surgery and treatment.
Summary:
NIFTP is a low grade thyroid neoplasm that has overlapping features with other thyroid neoplasms. The differences between it and other neoplasms are subtle and there is no single distinguishing feature. In order to diagnose it accurately, pathologists have to put all the morphological features and subtle unique features together. The unique features were a cellular aspirate with abundant small clusters and microfollicles similar to follicular adenoma, with slightly enlarged, crowded nuclei with frequent nuclear grooves, slightly clear chromatin, and mild irregular contours similar to papillary carcinoma. Colloid was often scant and dense. Ill-defined nuclear inclusions were noted in ~40% of cases but well-defined nuclear inclusions were infrequent.
Answers:
1. D
2. C
3. C
4. EReferences:
1. Yuri E. Nikiforov, MD, PhD et al. Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma. A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. JAMA Oncol. 2016;2(8):1023-1029.
2. Ghossein RA: Encapsulated malignant follicular cell-derived tumors. Endocr Pathol 2010; 21: 212–218.
3. Castro P, Rebocho AP, Soares RJ, et al: PAX8-PPARgamma rearrangement is frequently detected in the follicular variant of papillary thyroid carcinoma. J Clin Endocrinol Metab 2006; 91: 213–220.
4. Rivera M, Ricarte-Filho J, Knauf J, et al: Molecular genotyping of papillary thyroid carcinoma follicular variant according to its histological subtypes (encapsulated vs. infiltrative) reveals distinct BRAF and RAS mutation patterns. Mod Pathol 2010; 23: 1191–1200.
5. Seethala RR, Baloch ZW, Barletta JA, Khanafshar E, Mete O, Sadow PM, LiVolsi VA, Nikiforov YE, Tallini G, Thompson LD. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists. Mod Pathol. 2017 Oct 20.
6. Eyibilen A, Aladağ I, Güven M, KöseoğluRD: Surgical approach to encapsulated follicular variant of papillary thyroid carcinoma: a report of three cases (in Turkish). Kulak Burun Bogaz Ihtis Derg 2008; 18: 384–388.
7. Yang GCH, Fried KO, Scognamiglio T. Sonographic and cytologic differences of NIFTP from infiltrative or invasive encapsulated follicular variant of papillary thyroid carcinoma: A Review of 179 Cases. Diagn Cytopathol. 2017 Jun;45(6):533-541.
8. Strickland KC, Howitt BE, Barletta JA, et al. Suggesting the cytologic diagnosis of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): A retrospective analysis of atypical and suspicious nodules. Cancer. 2017 Sep 15.
9. Jaconi M, Manzoni M, Pincelli AI, et al. The impact of the non-invasive follicular thyroid neoplasm with papillary-like nuclear feature terminology in the routine diagnosis of thyroid tumours. Cytopathology. 2017 Sep 3.
10. Chandler JB, Colunga M, Prasad ML, et al. Identification of distinct cytomorphologic features in the diagnosis of NIFTP at the time of preoperative FNA: Implications for patient management. Cancer. 2017 Aug 21.
11. Brandler TC, Zhou F, Liu CZ, et al. Can noninvasive follicular thyroid neoplasm with papillary-like nuclear features be distinguished from classic papillary thyroid carcinoma and follicular adenomas by fine needle aspiration? Cancer Cytopathol. 2017; Jun; 126(6):378-388.
12. Bizzarro T, Martini M, Capodimonti S,et al. Young investigator challenge: the morphologic analysis of noninvasive follicular thyroid neoplasm with papillary-like nuclear features on liquid-based cytology: some insights into their identification. Cancer Cytopathol. 2016 Oct; 124(10):699-710.
13. Singh R, Avila J, Jo K, et al. Patients with on-invasive follicular thyroid neoplasm with papillary-like nuclear features are unlikely to have malignant preoperative cytology. Ann Surg Oncol. 2017 Oct 24(11):3300-3305.
14. Zhao L, Dias-santagata D, Sadow PM, et al. Cytological, molecular, and clinical features of noninvasive follicular thyroid neoplasm with papillary-like nuclear features versus invasive forms of follicular variant of papillary thyroid carcinoma. Cancer cytopathol 2017 May; 125(5):323-331.
15. Howitt BE, Chang S, Eszlinger M, et al. Fine-needle aspiration diagnoses of noninvasive follicular variant of papillary thyroid carcinoma. Am J Clin Pathol. 2015;144:850-857.
16. Maletta F, Massa F, Torregrossa L, et al. Cytological features of “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” and their correlation with tumor histology. Hum Pathol. 2016;54:134-142.Contributed by:
Zesong Zhang, MD,
Assistant Professor
Department of Pathology
Icahn School of Medicine at Mount Sinai
New York, NY 10029