Case of the Month ...
Clinical History: A 72-year-old woman underwent an endobronchial ultrasound-guided fine needle aspiration (FNA) of a 1.0 cm well-circumscribed mass.
Authors: Michelle Garlin Politis, Maelle Saliba, Niyati Desai, Anjali Saqi
Diagnosis & Discussion
click on image for larger version
Images 1-2:
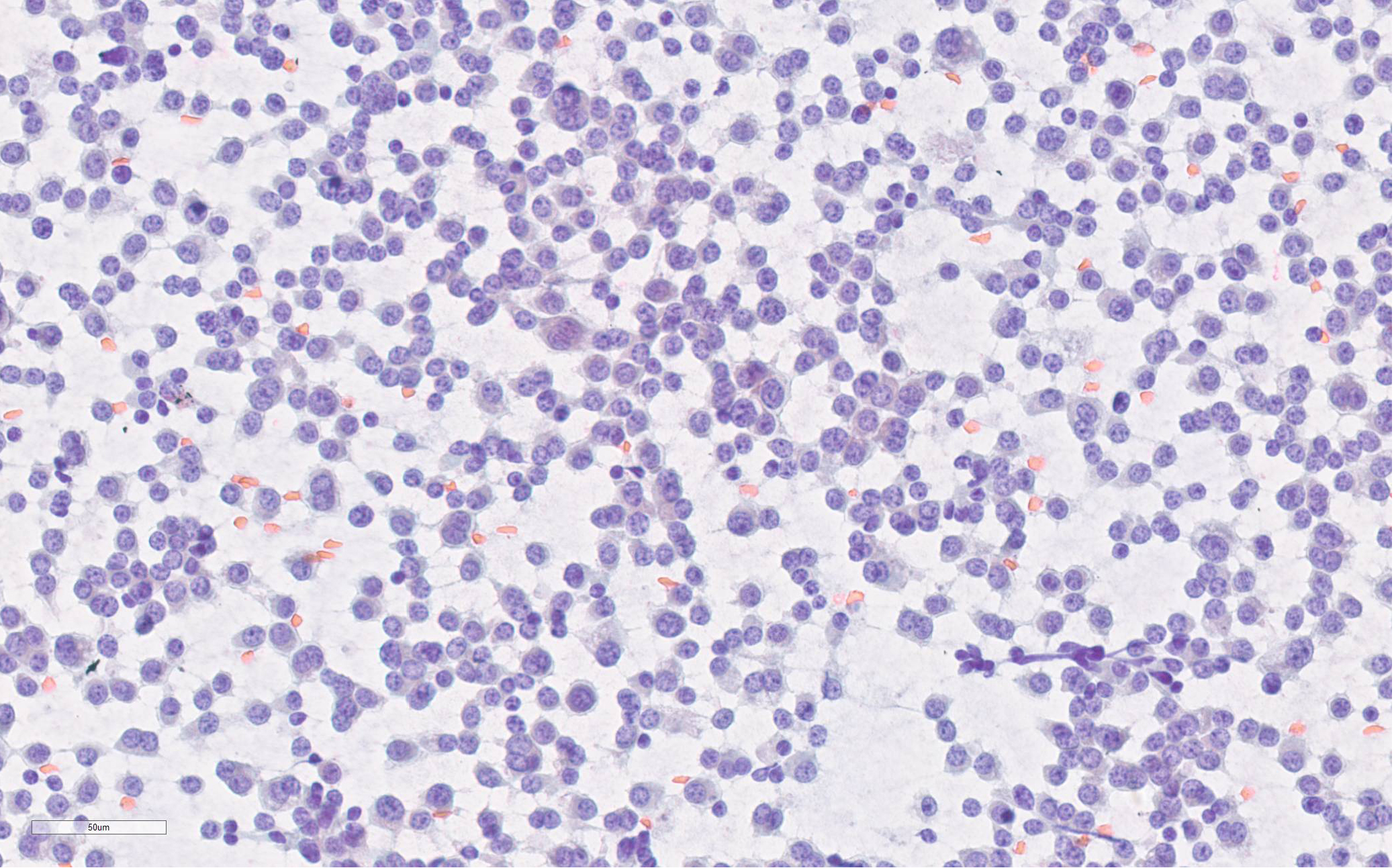
Figure 1: FNA of lung mass (Diff-Quik Stain 400x)
Figure 2: FNA of lung mass (Papanicolaou Stain 400x)
Questions:
- Q: A 72-year-old woman underwent an endobronchial ultrasound-guided fine needle aspiration (FNA) of a 1.0 cm well-circumscribed mass.
What is the best diagnosis based on the FNA images?
- Typical carcinoid
- Atypical carcinoid
- Carcinoid not otherwise specified (NOS)
- Small cell carcinoma
- Which of the following statements best describes typical and atypical carcinoids?
- PD-L1 testing is standard of care for typical and atypical carcinoids
- Typical and atypical carcinoids can only be definitively diagnosed on surgical resections
- CD56 is the most specific neuroendocrine marker
- INSM1 is the least sensitive and specific neuroendocrine marker
Answers:
Question 1: Correct answer is C
The distinction between typical (low-grade) and atypical (intermediate-grade) carcinoids is based on mitoses per 2 mm2 and punctate necrosis. Per the most recent 2021, 5th edition of World Health Organization (WHO) classification of thoracic tumors, cytology and small biopsy specimens with typical (<2 mitoses/2mm2; no necrosis) or atypical (2-10 mitoses/2mm2 and/or punctate necrosis) carcinoids should be reported as “carcinoid tumor, not otherwise specified (NOS).” This update also extends to metastases with recommended reporting as “metastatic carcinoid tumor, NOS.” The following represent the rationale for reclassification:
- Definitions of typical and atypical carcinoids were established for resection specimens
- Cytology and small biopsy represent limited tumor sampling precluding definitive distinction between the two entities (e.g., assessment of mitotic counts per 2 mm2), as assessment of mitotic counts per 2 mm2 may be underrepresented.
Question 2: Correct answer is B
A definitive diagnsis of typical or atypical carcinoid is reserved for surgically resected tumors. Currently, PD-L1 immunostaining is not standard of care for typical and atypical carcinoids.
CD56 is the most sensitive but least specific of neuroendocrine markers while INSM1 is a more sensitive and specific marker independent of the primary site.
References:
1. Sung S, Heymann JJ, Politis MG, Baine MK, Rekhtman N, Saqi A. Small Biopsy and Cytology of Pulmonary Neuroendocrine Neoplasms: Brief Overview of Classification, Immunohistochemistry, Molecular Profiles, and World Health Organization Updates. Adv Anat Pathol. 2022 Nov 1;29(6):329-336. doi: 10.1097/PAP.0000000000000360. Epub 2022 Sep 2. PMID: 36053019.
2. Rekhtman N. Lung neuroendocrine neoplasms: recent progress and persistent challenges. Mod Pathol. 2022;35(Suppl 1):36-50.3.WHO Classification of Tumours Editorial Board. Thoracic Tumours. 5th ed. Lyon (France): International Agency for Research on Cancer. (2021).
4.Rodriguez EF, Fite JJ, Chowsilpa S, Maleki Z. Insulinoma-associated protein 1 immunostaining on cytology specimens: an institutional experience. Hum Pathol. 2019;85:128-135. doi:10.1016/j.humpath.2018.10.03