Case of the Month ...
A 72-year-old male with a longstanding smoking history and chest CT demonstrating a 2-cm solid right middle/lower lobe perihilar region nodule abutting the oblique fissure and few scattered punctate 2 mm left and right lower lobe nodules. An endobronchial ultrasound guided fine needle biopsy of the dominant lung nodule and mediastinal lymph node were performed.
Authors
- Ragheb Rezko MD; Ramya Gadde, MD. Department of Pathology, University Hospitals Cleveland Medical Center, Case Western Reserve University, Cleveland, Ohio
Diagnosis & Discussion
click on image for larger version
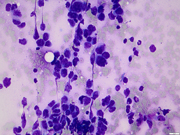
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
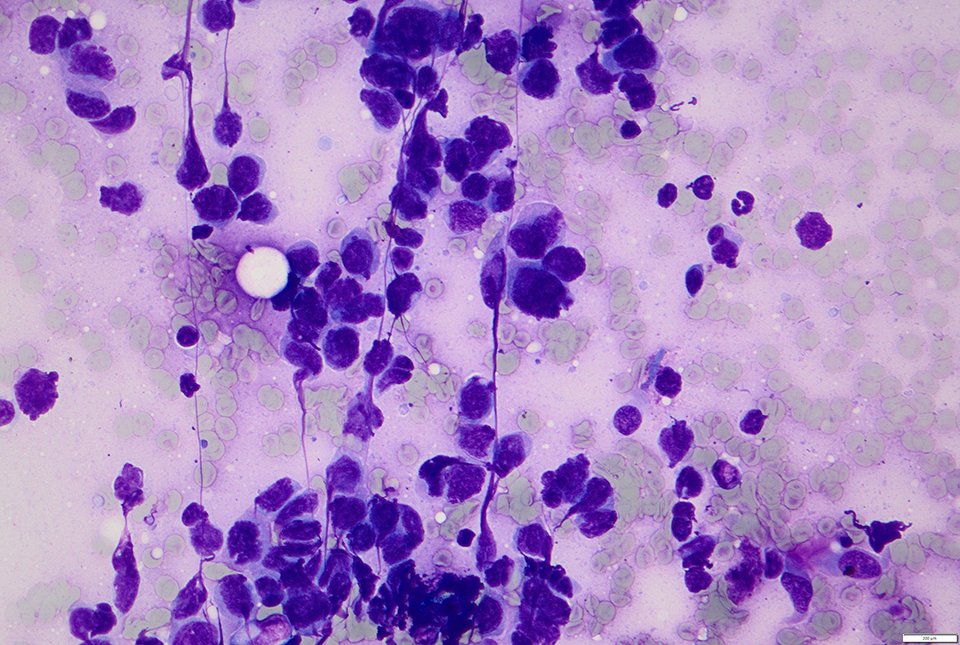
- Figure 1: Diff-Quik stain, 400x
- Figure 2: Diff-Quik stain, 600x
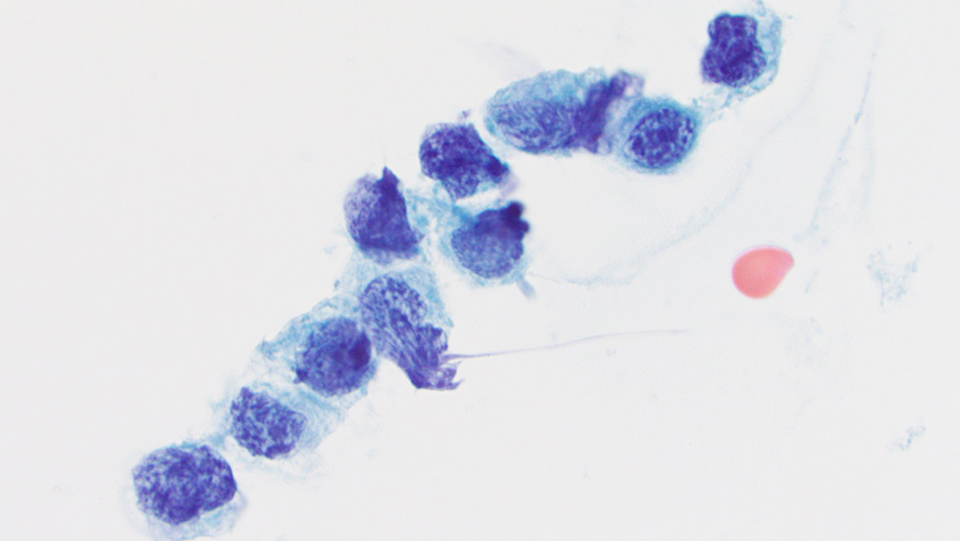
- Figure 3: Papanicolaou stain 1000x
- Figure 4: Cell Block, Hematoxylin and Eosin Stain, 400x.
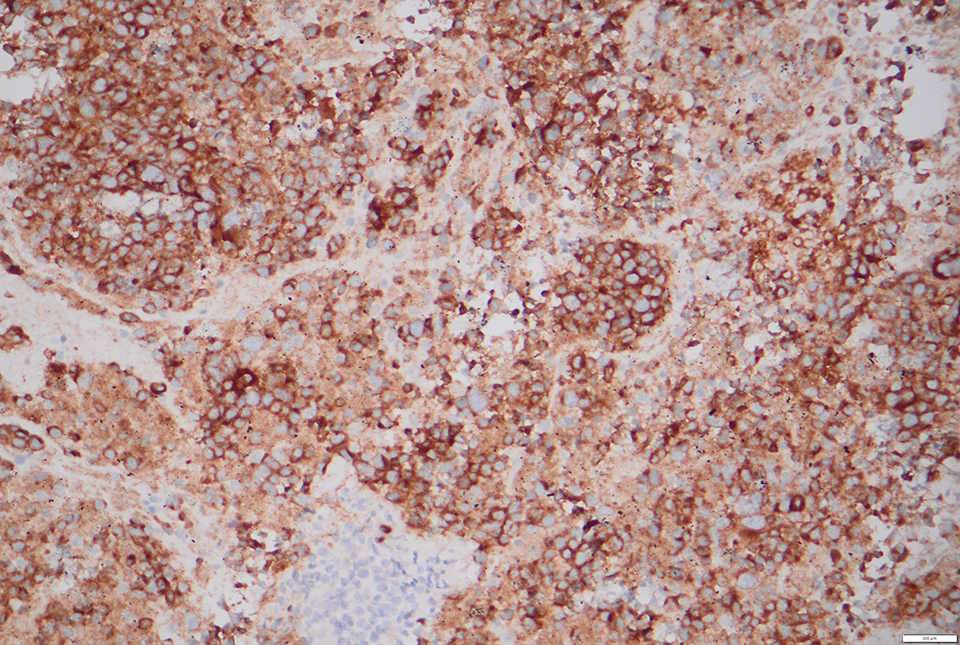
- Figure 5: Synaptophysin, 200x
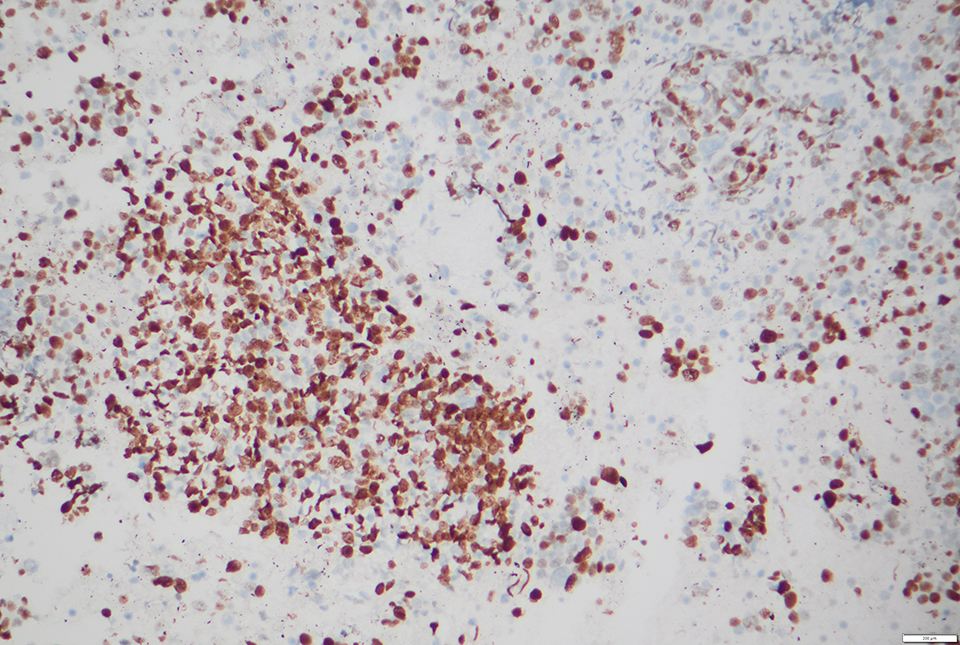
- Figure 6: Ki67, 200x
Additionally, neoplastic cells were positive for chromogranin and negative for TTF-1 and p40; RB1 was retained (images not shown).
Questions:
- Based on morphology and immunohistochemistry, which of the following is the best diagnosis?
- Small cell carcinoma
- Carcinoid not otherwise specified (NOS)
- Large cell neuroendocrine carcinoma
- Non-small cell carcinoma
- Which of following features favors large cell neuroendocrine carcinoma over small cell carcinoma?
- Moderate cytoplasm
- Nuclear molding
- High mitotic rate (>10 mitoses/2 mm2)
- Necrosis
Answers:
Question 1: Correct answer is C
Question 2: Correct answer is A
Discussion:
Large cell neuroendocrine carcinoma (LCNEC) is a rare pulmonary malignancy associated with smoking and a poor 5-year prognosis.1,2 Both small cell carcinoma (SCLC) and LCNEC represent high-grade neuroendocrine tumors and have similarities, but key cytomorphological features distinguish the two.
By definition, SCLC and LCNEC have necrosis and high mitotic activity (>10 mitoses/2mm2). Like SCLC, LCNEC can present in combination with non-small cell carcinoma (e.g., adenocarcinoma or squamous cell carcinoma). Also, the genetic profile of LCNEC may be similar to that of SCLC (i.e., TP53, RB1, MYCL) or have adenocarcinoma-like mutations (e.g., KRAS).3
LCNEC has neuroendocrine architecture (e.g., nested, trabecular, rosette). In contrast to SCLC, LCNEC cells are intermediate to large with moderate-to-abundant granular cytoplasm, frequently show nuclei with coarse chromatin and prominent nucleoli. By 2021 WHO criteria, LCNEC must stain with at least one neuroendocrine marker (e.g., chromogranin, synaptophysin, CD56).2
Per 2021 WHO classification of lung tumors, LCNEC may be diagnosed on cytology and small biopsy specimens when morphological and immunohistochemical criteria are satisfied.2 However, per 2022 cytopathology WHO criteria, LCNEC definitive diagnosis is difficult in cytology samples but can be suggested in cases with cellular cell blocks that allow the assessment of morphological and immunohistochemical criteria.1 In cases where the features overlap with small cell, the recommendation is that it is reported as high-grade neuroendocrine carcinoma, with features suggestive of LCNEC. If scant sampling limits fulfillment of both, a diagnosis of “non-small cell lung carcinoma, possible large cell neuroendocrine carcinoma” is the preferred terminology.1,2
TTF-1 is expressed in a subset of LCNEC, and Napsin-A is commonly negative. While Ki-67 is high (> 40%) and useful in small samples to distinguish from carcinoid, its use is not essential for LCNEC diagnosis.
Systemic treatment for advanced LCNEC is variable—both SCLC and non-small cell lung carcinoma options are used. 2REFERENCES
- Schmitt FC, Bubendorf L, Canberk S, Chandra A, Cree IA, Engels M, Hiroshima K, Jain D, Kholová I, Layfield L, Mehrotra R, Michael CW, Osamura R, Pitman MB, Roy-Chowdhuri S, Satoh Y, VanderLaan P, Zakowski MF, Field AS. The World Health Organization Reporting System for Lung Cytopathology. Acta Cytol. 2023;67(1):80-91. doi: 10.1159/000527580. Epub 2022 Dec 12. PMID: 36509066.
- Andrew G. Nicholson, Ming S. Tsao, Mary Beth Beasley, Alain C. Borczuk, Elisabeth Brambilla, Wendy A. Cooper, Sanja Dacic, Deepali Jain, Keith M. Kerr, Sylvie Lantuejoul, Masayuki Noguchi, Mauro Papotti, Natasha Rekhtman, Giorgio Scagliotti, Paul van Schil, Lynette Sholl, Yasushi Yatabe, Akihiko Yoshida, William D. Travis, The 2021 WHO Classification of Lung Tumors: Impact of Advances Since 2015, Journal of Thoracic Oncology, Volume 17, Issue 3, 2022, Pages 362-387, ISSN 1556-0864.
- Rekhtman N, Pietanza M.C, Hellmann M.D, et al. Next-generation sequencing of pulmonary large cell neuroendocrine carcinoma reveals small cell carcinoma-like and non-small cell carcinoma-like subsets. Clin Cancer Res . 2016;22(14):3618–3629.