Case of the Month ...
A 68-year-old male, former smoker, with a medical history of paraplegia due to a gunshot wound, and atrial fibrillation (managed with warfarin), presented with haemoptysis and intermittent shortness of breath. A chest CT angiography incidentally revealed a right hilar mass measuring 2.5 cm. A PET scan indicated that the hilar mass was mildly hypermetabolic, yet there was no evidence of hypermetabolic lymphadenopathy or distant hypermetabolic disease anywhere else. He then underwent an endoscopic ultrasound evaluation, during which fine needle aspiration was performed on the hilar mass.
Authors
Harpreet Virk, Omid Savari. Department of Pathology. University Hospitals Cleveland Medical Center. Case Western Reserve University, Cleveland, OH
Diagnosis & Discussion
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Figure 7 Images 1-7:
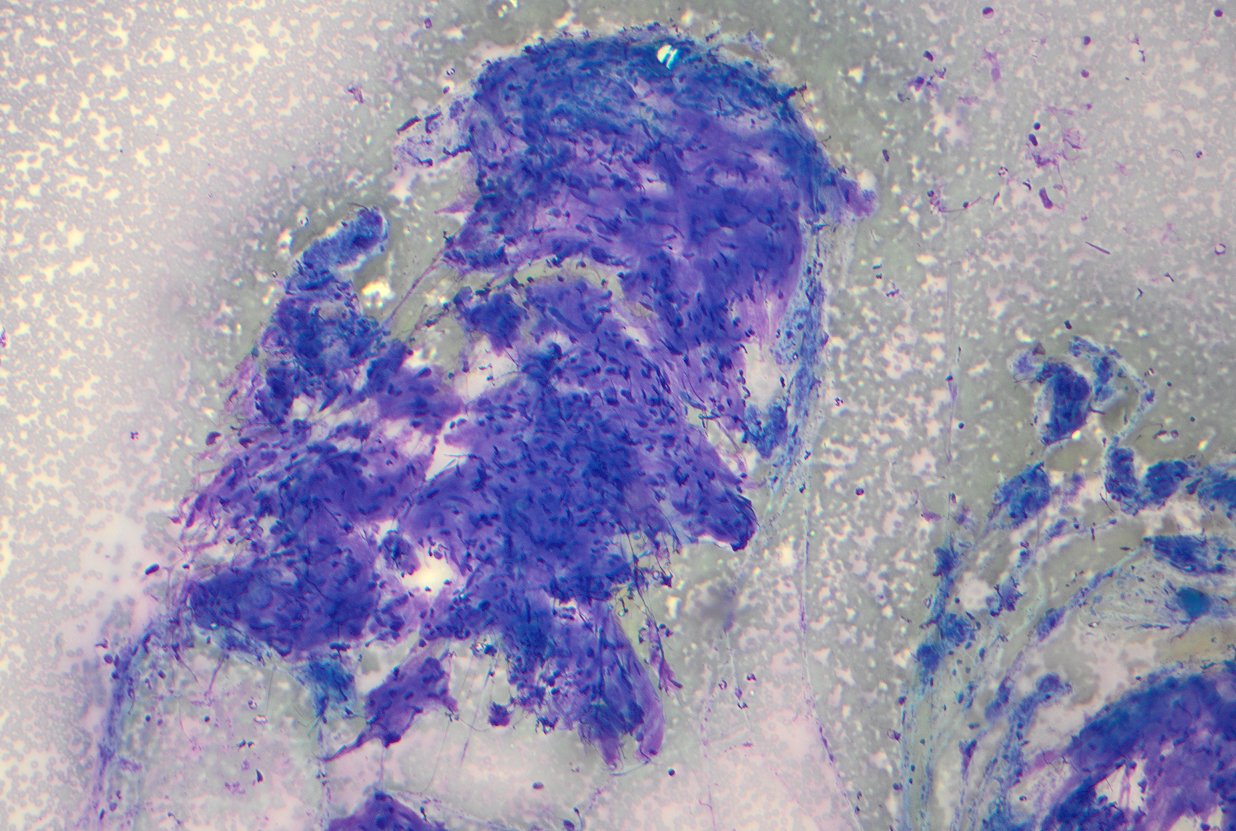
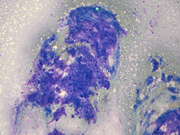
Figure 1: EBUS FNA of hilar mass, aspirate smear, Diff-Quik stained
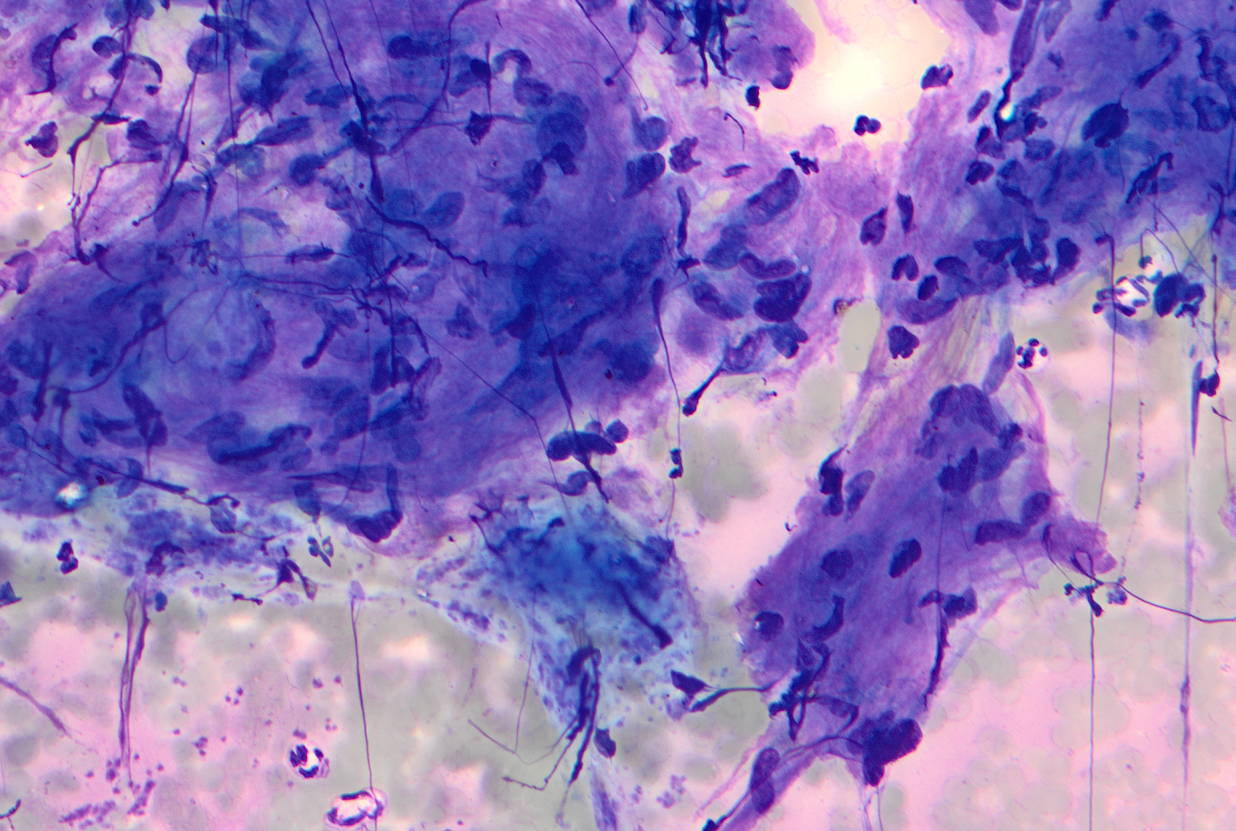
Figure 2: EBUS FNA of hilar mass, aspirate smear, Diff-Quik stained
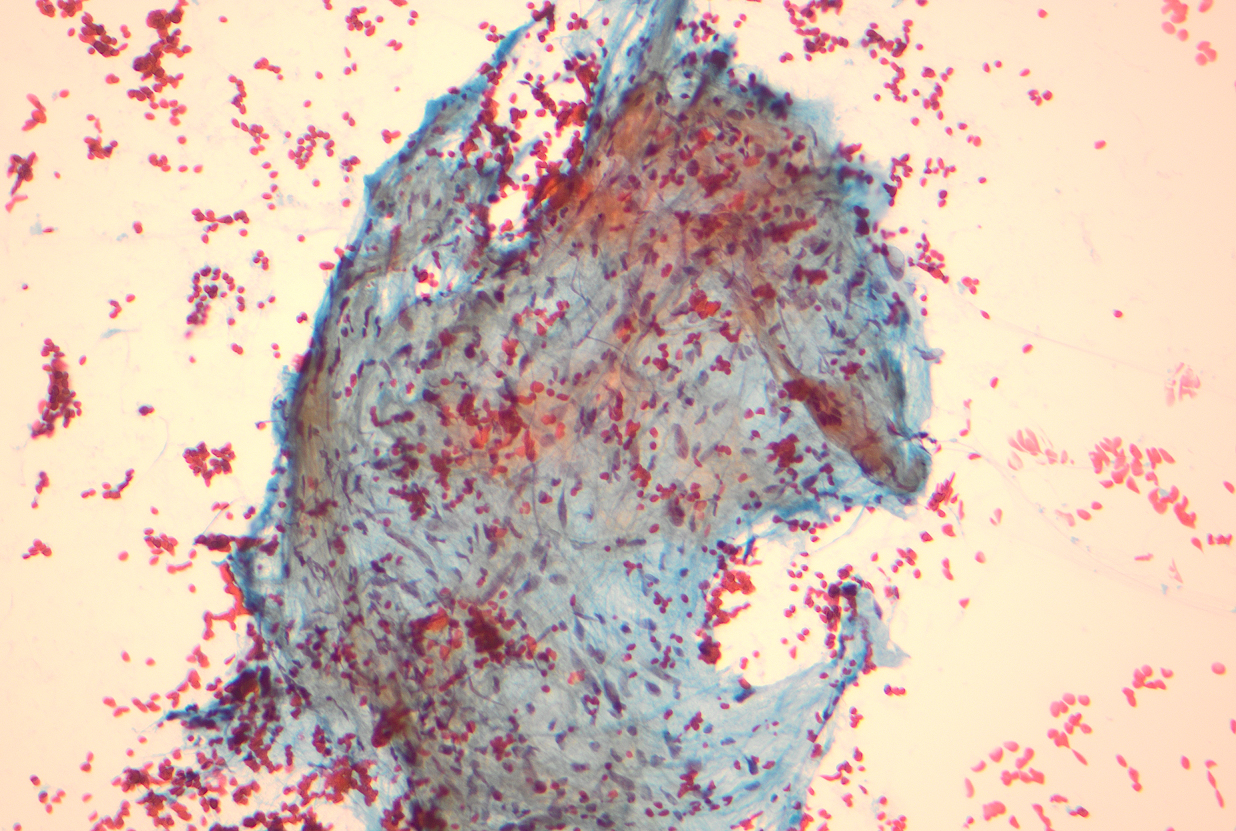
Figure 3: EBUS FNA of hilar mass, aspirate smear, PAP stained
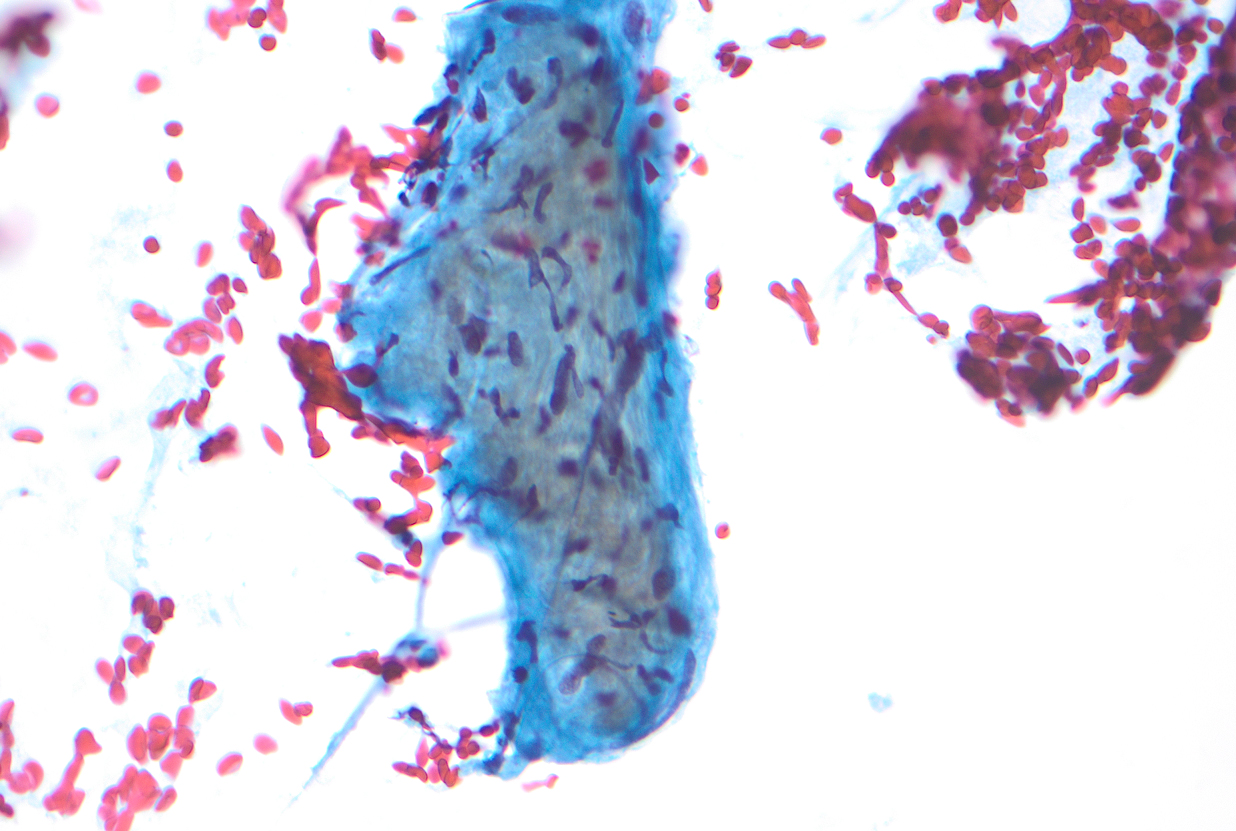
Figure 4: EBUS FNA of hilar mass, aspirate smear, PAP stained
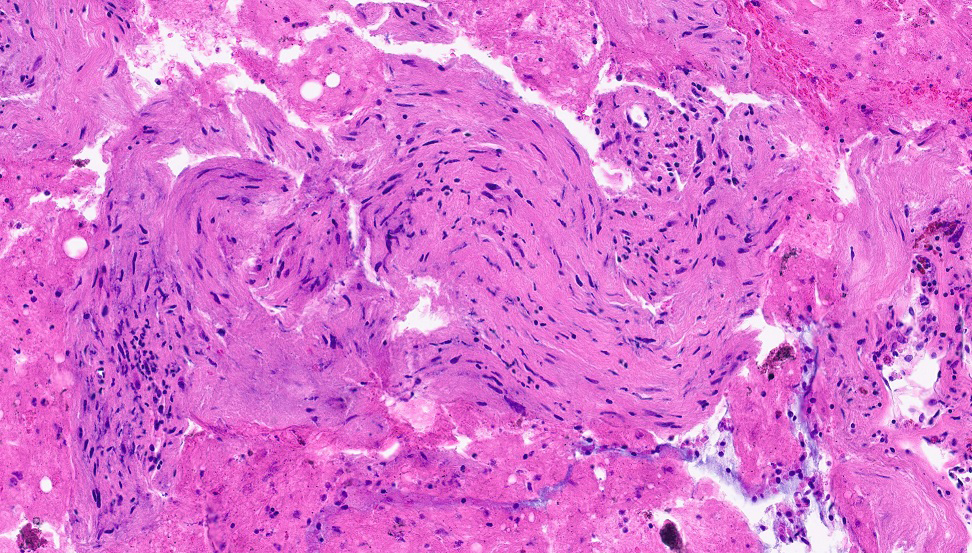
Figure 5: Cell block, Hematoxylin and Eosin (H&E) stain
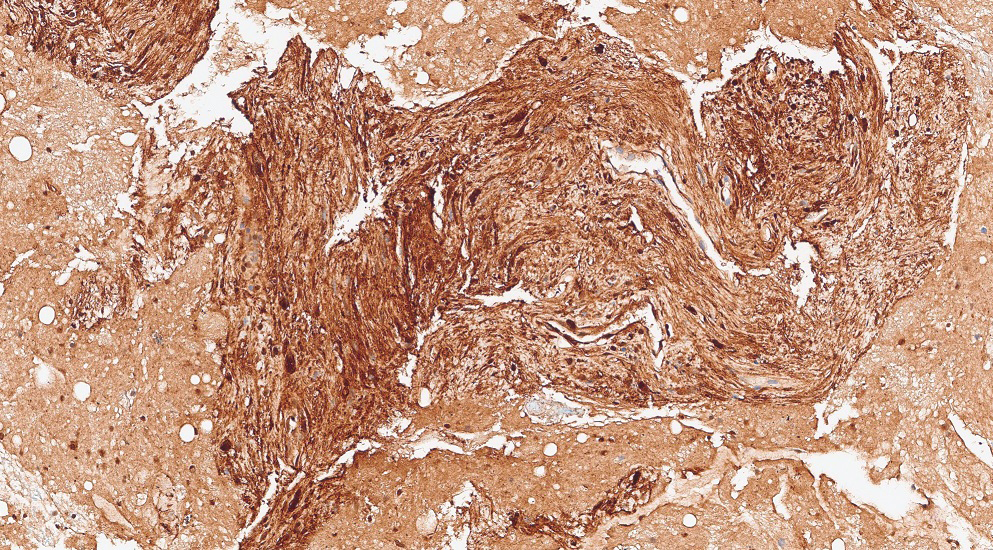
Figure 6: Cell block, S100 immunocytochemical stain
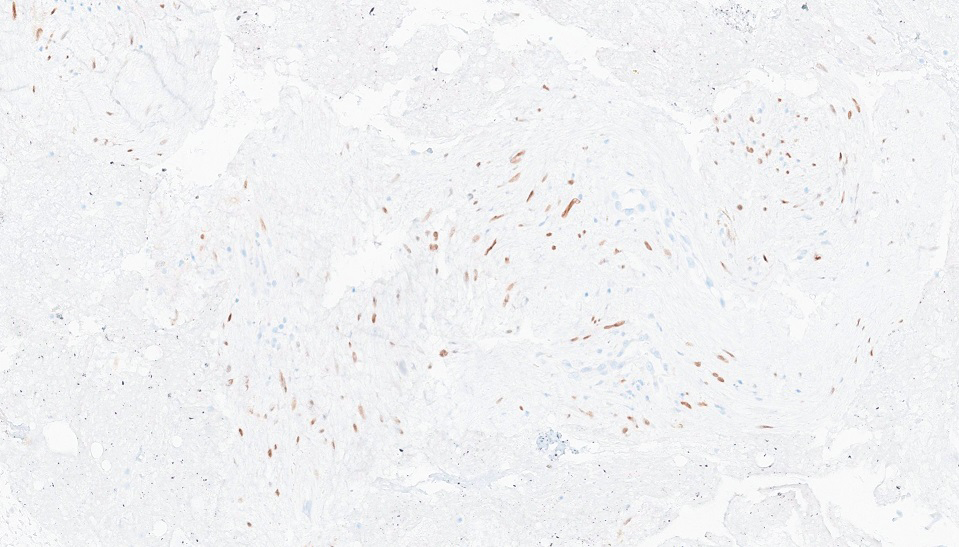
Figure 7: Cell block, SOX10 immunocytochemical stainQuestions:
- What is the best diagnosis based on cytomorphology and immunocytochemical stain (Figure 1 to 6)?
- Pleomorphic Carcinoma
- Lieomyosarcoma
- Schwannoma
- Pulmonary Hamartoma
- Solitary Fibrous Tumour
- Which of the following morphological features is NOT regarded as a key characteristic of this neoplasm?
- Nuclear palisading
- Buckled nuclei with tapered ends
- Fibrotic or myxoid stroma
- Bland ovoid nuclei with blunt ends
- Mild pleomorphism and mitotic activity
- Which of the following combination of immunocytochemical stains are expected to show characteristic positivity in this entity?
- Cytokeratin AE1/AE3 and SMA
- S100 and DOG1
- SOX10 and S100
- S100 and CD34
- SOX10 and CD117
Answers:
Question 1: Correct Answer is C
The FNA aspirate smears (Figure 1 to 4) show clusters of spindle shaped cells arranged in short fascicles with pale eosinophilic cytoplasm, and slender wavy or buckled nuclei. No significant nuclear atypia, mitotic activity or necrosis was identified. Variable amount of collagenous material separates these spindle cells. The cell block (Figure 5) shows cohesive tissue fragments, with fibrillary stroma and focal palisading of the spindle, wavy, or fish-hook–like nuclei with pointed ends. The spindle cells show fine chromatin, smooth and regular nuclear membranes, and inconspicuous nucleoli and bipolar spindle cytoplasm. Immunocytochemical stain performed on the cell block reveals that spindle cells are positive for S-100 (Figure 6). The cells also showed nuclear positivity for SOX-10, while they were negative for cytokeratin AE1/3 and CAM5.2, CD68, CD34, CD117, DOG1, ERG, MelanA, and HMB45 (Not shown).
Schwannomas in the thoracic cavity typically arise in the posterior mediastinum, near the paravertebral region, but can also occur in other mediastinal compartments or the pleura. These slow-growing, solitary tumors are usually asymptomatic and are often discovered incidentally on imaging or at autopsy.
Schwannomas can be challenging to differentiate from other spindle cell tumors on cytopathological smears (Table 1). Correlation with clinical history, imaging, and location is essential, and immunocytochemistry (ICC) on cell blocks and core needle biopsies serves as a valuable adjunct.Question 2: Correct Answer is D
The conventional schwannomas are spindle cell neoplasms with alternating Antoni A (compact) and Antoni B (hypocellular) patterns. Verocay bodies, characterized by nuclear palisading, may be present. The spindle cells have pale eosinophilic cytoplasm and ovoid or tapered nuclei. Some tumors exhibit cytoplasmic nuclear pseudoinclusions, mild pleomorphism, and mitotic activity. Ancient schwannomas show scattered atypical or bizarre nuclei with dark, smudgy chromatin, indicating degenerative changes.
Leiomyomas are characterized by bland, ovoid nuclei with blunt ends (cigar-shaped), while schwannomas have a more pointed ends.Question 3: Correct Answer is C
All schwannomas show diffuse nuclear and cytoplasmic staining for S100, particularly in Antoni A (Cellular) areas. SOX10 nuclear staining is usually extensive. GFAP and CD34 staining is variable. Mediastinal schwannomas can show patchy staining for cytokeratin AE1/AE3. Table 1 highlights the characteristic ICC in other spindle cell lesions in differential diagnosis.
References:
- Domanski HA, Akerman M, Engellau J, Gustafson P, Mertens F, Rydholm A. Fine-needle aspiration of neurilemoma (schwannoma). A clinicocytopathologic study of 116 patients. Diagn Cytopathol. 2006 Jun;34(6):403-12. doi: 10.1002/dc.20449.
- Chebib I, Hornicek FJ, Nielsen GP, Deshpande V. Cytomorphologic features that distinguish schwannoma from other low-grade spindle cell lesions. Cancer Cytopathol. 2015 Mar;123(3):171-9. doi: 10.1002/cncy.21506.
- Dahl I, Hagmar B, Idvall I. Benign solitary neurilemoma (Schwannoma). A correlative cytological and histological study of 28 cases. Acta Pathol Microbiol Immunol Scand A. 1984 Mar;92(2):91-101.
- Nonaka D, Chiriboga L, Rubin BP. Sox10: a pan-schwannian and melanocytic marker. Am J Surg Pathol. 2008 Sep;32(9):1291-8. doi: 10.1097/PAS.0b013e3181658c14.
- Karamchandani JR, Nielsen TO, van de Rijn M, West RB. Sox10 and S100 in the diagnosis of soft-tissue neoplasms. Appl Immunohistochem Mol Morphol. 2012 Oct;20(5):445-50. doi: 10.1097/PAI.0b013e318244ff4b.
- Boland JM, Colby TV, Folpe AL. Intrathoracic peripheral nerve sheath tumors-a clinicopathological study of 75 cases. Hum Pathol. 2015 Mar;46(3):419-25. doi: 10.1016/j.humpath.2014.11.017.
- Serrano C, George S. Leiomyosarcoma. Hematol Oncol Clin North Am. 2013 Oct;27(5):957-74. doi: 10.1016/j.hoc.2013.07.002.
- Wick MR. Hamartomas and other tumor-like malformations of the lungs and heart. Semin Diagn Pathol. 2019 Jan;36(1):2-10. doi: 10.1053/j.semdp.2018.11.002.
- Hupp M, Najmuddin M, Dincer HE, Mallery JS, Amin K, Stewart J 3rd. Cytomorphologic features of malignant solitary fibrous tumor with mediastinal involvement sampled by endoscopic and endobronchial ultrasound-guided fine-needle aspiration: A comparison of two cases. Diagn Cytopathol. 2019 Aug;47(8):821-827. doi: 10.1002/dc.24192.
- Choi HS, Seol H, Heo IY, Jung CW, Cho SY, Park S, Koh JS, Lee SS. Fine-needle aspiration cytology of pleomorphic carcinomas of the lung. Korean J Pathol. 2012 Dec;46(6):576-82. doi: 10.4132/KoreanJPathol.2012.46.6.576.