Case of the Month ...
A 61-year-old female presented for routine annual physical examination and was incidentally found to have a pulmonary nodule on CT imaging intended for coronary artery calcium scoring. Dedicated CT chest revealed a 13 x 10 mm solid, well-circumscribed, non-calcified nodule in the central right lower lobe of the lung. There was no evidence of additional pulmonary nodules, lymphadenopathy, or pleural effusion. The patient was asymptomatic from a pulmonary standpoint, denying cough, shortness of breath, wheezing, hemoptysis, or chest pain. The patient subsequently underwent endobronchial ultrasound guided fine needle aspiration of the lesion in pursuit of a diagnosis.
Authors
- Kelsey McHugh, MD – Mayo Clinic Arizona
Diagnosis & Discussion
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
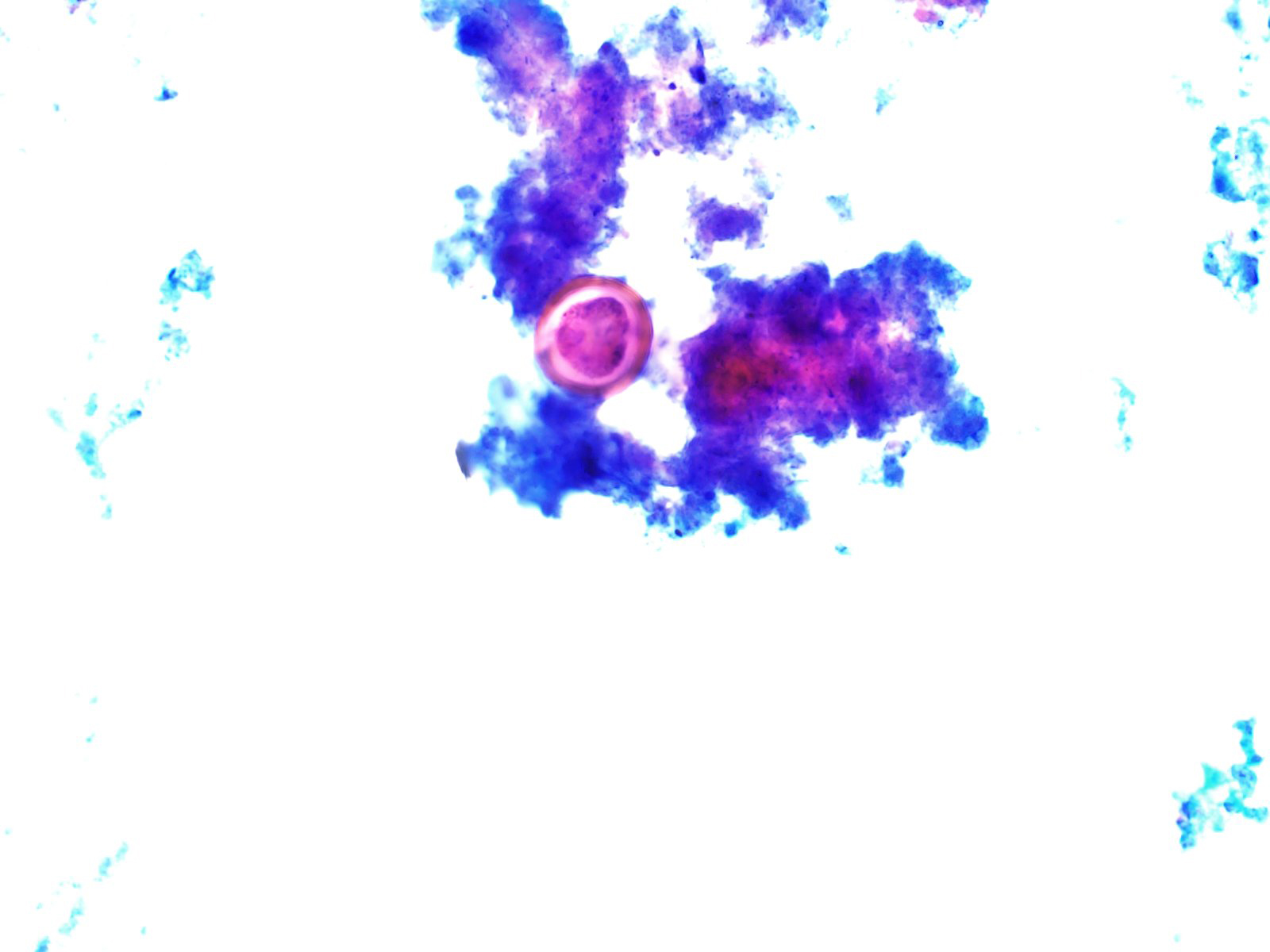
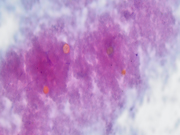
Figure 1: EBUS FNA of right lower lobe nodule, aspirate smear, Pap stained, 400x magnification.
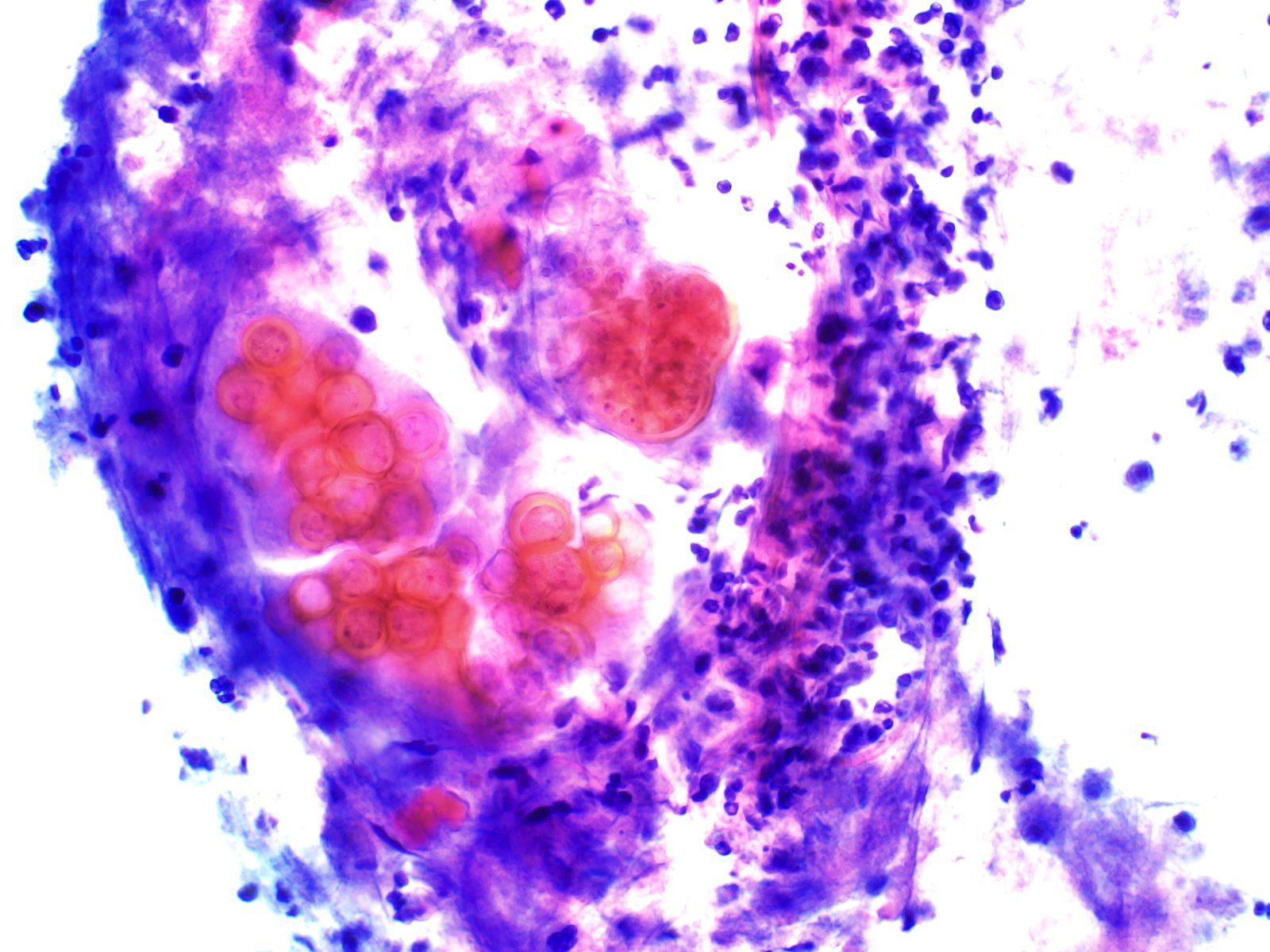
Figure 2: EBUS FNA of right lower lobe nodule, aspirate smear, Pap stained, 600x magnification.
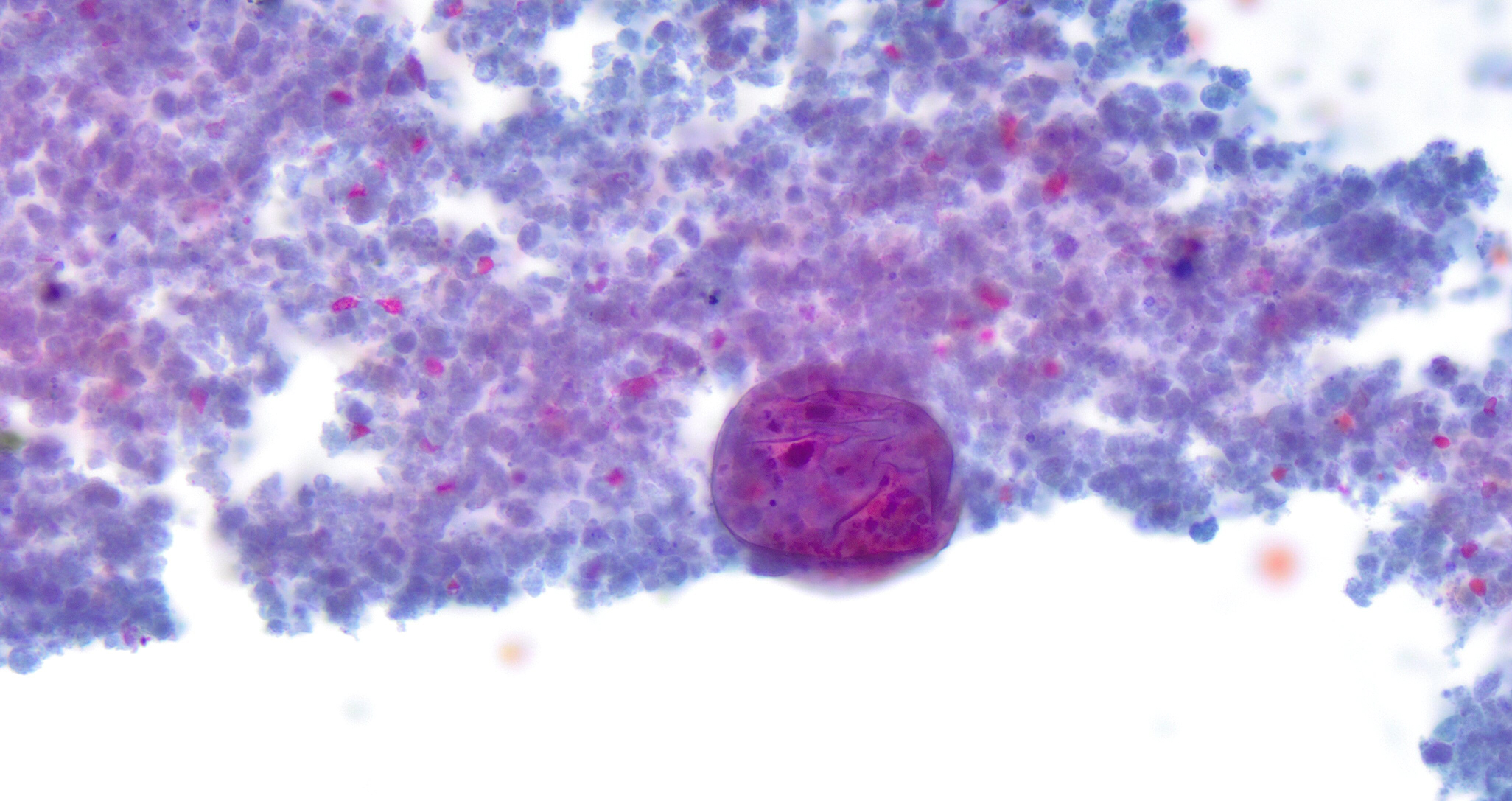
Figure 3: EBUS FNA of right lower lobe nodule, aspirate smear, Pap stained, 400x magnification.
Figure 4: EBUS FNA of right lower lobe nodule, aspirate smear, Pap stained, 600x magnification.
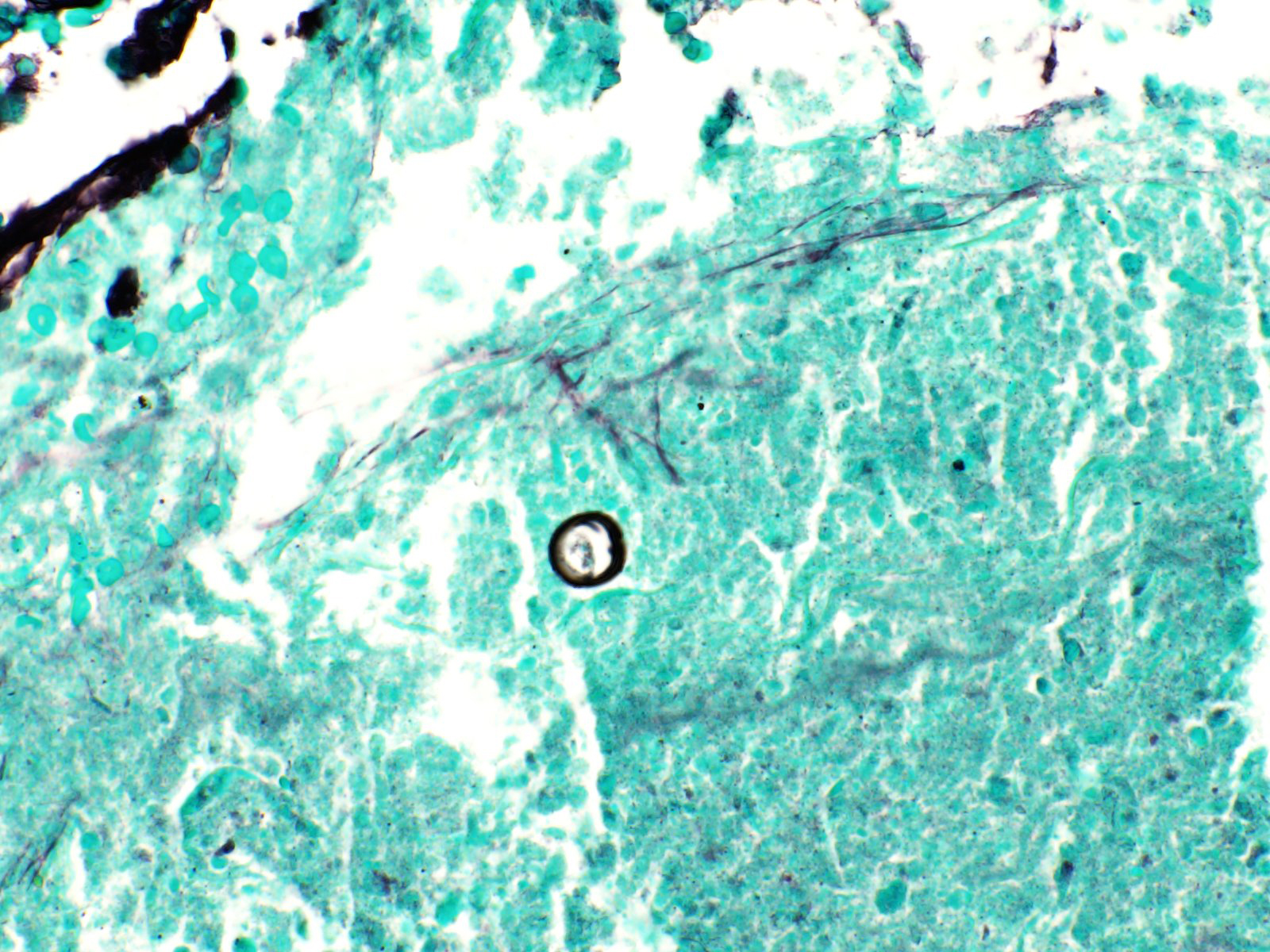
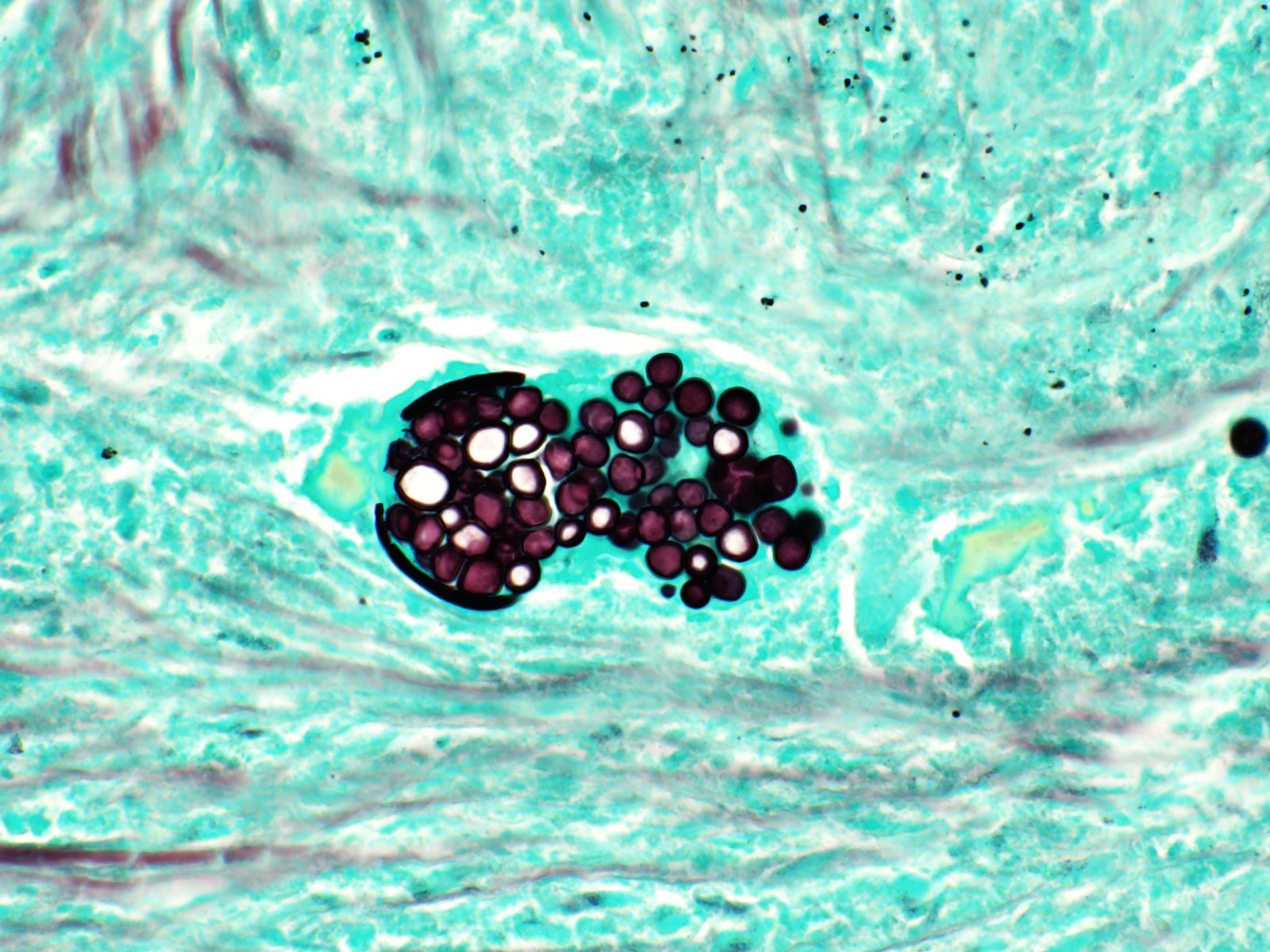
Figure 5: EBUS FNA of right lower lobe nodule, cell block, GMS, 400x magnification.
Figure 6: EBUS FNA of right lower lobe nodule, cell block, GMS, 400x magnification.
Questions:
- What is the best diagnosis based on the cytomorphology in Figures 1 through 6?
- Adenocarcinoma
- Paracoccidioidomycosis
- Histoplasmosis
- Coccidiodomycosis
- HSV infection
- What are the three endemic mycoses found in the North America?
- Histoplasmosis, Coccidioidomycosis, Blastomycosis
- Coccidioidomycosis, Sporothrix, Blastomycosis
- Histoplasmosis, Cryptococcosis, Blastomycosis
- Coccidioidomycosis, Paracoccidioidomycosis, Histoplasmosis
- Histoplasmosis, Paracoccidioidomycosis , Blastomycosis
- What is the most common clinical presentation of Coccidioides infection?
- Acute respiratory illness
- Asymptomatic
- Progressive or disseminated disease
- Nasea and vomiting
- Pulmonary nodules
Answers:
Question 1: Correct answer is D
Coccidioides fungal organisms consist of a heterogeneous collection of spherules that vary widely in size, typically ranging from 2 to 20 mm. As this fungus replicates, the spherules grow larger and become endosporulating spheres that contain innumerable small endospores (2 to 4 mm). The large endosporulating forms can measure up to 200 mm. These endosporulating forms do eventually rupture, spilling their endospores and subsequently restarting the lifecycle with endospores that begin to mature into a heterogeneous collection of variably sized spherules. Beyond endospores, immature spherules and endosporulating spherules, Coccidioides can also exist as hyphae and arthroconidia, with these two forms most typically restricted to within the environment. Hyphal forms of Coccidioides are uncommon to see in vivo, serving as a major diagnostic pitfall in the rare instances they are encountered. Coccidioides arthroconidia are 3 to 5 mm ovoid-type structures that, once inhaled, round up to become a immature spherules. Generally, regardless of body site, Coccidioides species are seen in a background of granulomatous inflammation with or without associated necrosis. On Papanicolaou stain, the spherules are orangeophilic. On Geimsa stain, they are generally transparent, appearing as negative images without significant staining. PAS stain highlights the spherules magenta and they appear as black spherules with or without a clear center on GMS.
Features that help discern Coccidioides from other fungal infections include organism size, organism shape, type of organism budding, and organism staining characteristics. See below Table 1 for further details in discerning between Coccidioides, Histoplasma, Blastomyces and Cryptococcus based on organism cytomorphology.Question 2: Correct answer is A
Endemic fungal species are those that are thermally dimorphic, have a limited geographic range, and are capable of causing both primary disease and opportunity infections. North, Central and South America have the largest number of endemic fungal species in the world, with North America being home to Histoplasma, Coccidioides and Blastomyces. The prototypical geographic distribution of Histoplasma in the United States is in central and eastern states, particularly those around the Ohio and Mississippi River Valleys. The prototypical geographic distribution of Blastomyces in the United States is in midwestern, south-central and southeastern states, particularly around the Ohio and Mississippi River Valleys, Great Lakes and Saint Lawrence River.
Regarding Coccidioides, there are two species: C. immitis and C. posadasii. These two species have slightly different geographic distributions, with C. immitis restricted to within southwestern North America and C. posadasii spanning from southwestern North America through Central America and into South America. Both species cause the same infectious disease within humans. These Coccidioides organisms exist in greatest density within the southwestern United States, particularly in Southern Arizona & Southern California. The term “Valley Fever” is actually derived from their prevalence within the San Joaquin Valley in Southern California. In the United States, it is estimated there are roughly 350,000 cases of coccidioidomycosis diagnosed annually, with the general trend being an increase in annual cases over the last 5-10 years. These fungal organisms can also be found within Mexico, Central America and parts of South America, with endemic areas identified within countries including Guatemala, El Salvador, Nicaragua, Honduras, Colombia, Venezuela, northeast Brazil, and northern Argentina.Question 3: Correct answer is B
In humans, Coccidioides is considered both a primary and an opportunistic fungal pathogen that occurs in both immunocompetent and immunocompromised individuals. Clinically, the majority of Coccidioides infections are asymptomatic (approximately 60-75% of cases). If symptomatic (approximately 25-40% of cases), infections are generally self-limited, with the host immune system resolving the infection without need for medical intervention. In these cases, the typical clinical presentation is that of a community acquired pneumonia, with a flu-like presentation that develops about 3 weeks after inoculation. Uncommonly, Coccidioides infection may present as a chronic progressive infection that results in the formation of pulmonary nodules or cavitary lesions. This is estimated to occur in about 5-7% of those who present with an acute respiratory illness. Very rarely, extrapulmonary dissemination may occur, most commonly to the joints & bones. Progressive or disseminated disease is estimated to occur in <2% of infections. Other sites more frequently involved in disseminated coccidioidomycosis include the central nervous system, skin and muscles. Coccidioides meningitis is generally the most severe complication of this infection and disseminated coccidioidomycosis has been reported to have a fatality rate of roughly 30%. The main risk factors for symptomatic infection can be grouped into endemic, occupational, and host-related risks. Endemic risk factors include residence in or travel to endemic areas. Occupational risk factors include activities with soil exposure, such as agriculture and construction. Host-related risk factors are anything that results in immunosuppression or immunocompromise, including drugs/medication and being in your third trimester of pregnancy.
Table 1. Characteristic Cytologic Features of Common Fungal Yeasts
OrganismSize
Shape
Budding
Useful Stains
Histoplasma
2 to 4 mm
Ovoid, small
Narrow halo due to retraction artifactSingle
Narrow-basedGMS: helpful when scant number of yeasts
Cryptococcus
5 to 20 mm
Round
Clear capsular haloSing
Narrow-based
Teardrop-shapedMucicarmine, PAS, Alcian blue: thick mucopolysaccharide capsule
Blastomyces
8 to 20 mm
Round, large
Double-contoured cell wallSingle
Broad-basedPap stain: blue-green yeast
Coccidioides
20 to 200 mm
Round, large
Thick-walled refractile spherulesEndospores (2-4 mm)
Pap stain: orangeophilic spherules
References:
Raab SS, Silverman JF, Zimmerman KG. Fine-Needle Aspiration Biopsy of Pulmonary Coccidioidomycosis: Spectrum of Cytologic Findings in 73 Patients. Am J Clin Pathol. 1993;99:582-587.
Ashraf N, Kubat RC, Poplin V, et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia. 2020;185:843-865.
Aly ZF, Millius R, Sobonya R, Aboul-Nasr K, Klein R. Cytologic Diagnosis of Coccidiomycosis: Spectrum of Findings in Southern Arizona Patients Over a 10 Year Period. Diagn Cytopathol. 2016;44:195-200.
George B, Rolon MDMR, Clement CG. Role of fine-needle aspiration cytology in early diagnosis of fungal infections. Diagn Cytopathol. 2020;48:645-651.
Van Dyke MCC, Thompson GR 3rd, Galgiani JN, Barker BM. The Rise of Coccidioides: Forces Against the Dust Devil Unleashed. Front Immunol. 2019;10:2188.