Case of the Month ...
A 41-year-old male presented with a one-year history of a painful left upper arm lesion. Ultrasonographic examination revealed a well-defined oval hyperechoic to isoechoic mass, measuring 2.1 cm in size, located between muscle bundles. FNA was performed.
Authors
- Daisy Sun, MD PhD, Miami Valley Hospital, Dayton, OH
- Mia Wang, The Seven Hills School, Cincinnati, OH
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
Figure 1: Rapid on-site evaluation (ROSE) FNA material of the left upper arm lesion, smear, Diff-Quik stain, 100x magnification.
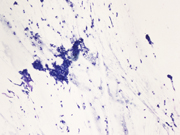
Figure 2: Rapid on-site evaluation (ROSE) FNA material of the left upper arm lesion, smear, Diff-Quik stain, 200x magnification.
Figure 3: Rapid on-site evaluation (ROSE) FNA material of the left upper arm lesion, smear, Diff-Quik stain, 200x magnification.
Figure 4: Rapid on-site evaluation (ROSE) FNA material of the left upper arm lesion, smear, Diff-Quik stain, 400x magnification.
Figure 5: FNA material of the left upper arm lesion, Cell Block, H&E, 200x magnification.
Figure 6: FNA material of the left upper arm lesion, Cell Block, SMA immunohistochemistry, 200x magnification.Questions:
What is the diagnosis?
- Paraganglioma
- Neuroendocrine tumor
- Glomus tumor
- Dermal nevus
- Which of the following statements is true about a benign glomus tumor?
- Complete surgical excision is curative
- It may metastasize in about 30% of cases
- It will show diffuse positivity for CD34, CD31 and ERG
- The most common location is in the stomach
- Which of the following molecular aberrations is most often seen in glomus tumors?
- ETV6-NTRK3
- EWSR1-FLI1
- MIR143-NOTCH1
- SS18-SSX2
Answers:
Question 1: Correct answer is C
The smears (Figures 1-4) show a cellular lesion composed of uniform round-to-oval cells in tight and loose cohesive clusters admixed with strands of magenta-colored material reminiscent of basement membrane. Spindled endothelial cells might be imagined in the periphery or crossing the cell clusters. The cell block material (Figure 5) shows uniformly rounded cells with punched-out nuclei, evenly dispersed nuclear chromatin with inconspicuous nucleoli, and eosinophilic cytoplasm growing around blood vessels. Immunohistochemistry performed on the cell block materials shows that the cells of interest are diffusely positive for SMA (Figure 6), while negative for AE1/3, synaptophysin, chromogranin, S100, and CD31. Ki-67 is very low. The cytologic findings are classic for glomus tumor (GT).
Question 2: Correct answer is A
GTs are rare mesenchymal tumors composed of modified smooth muscle cells that arise from the glomus body, with an estimated incidence of about 1.5% of soft tissue tumors. The glomus body resides in the stratum reticularis of the dermis and visceral organs. The normal glomus body is a specialized form of an arteriovenous anastomosis that primarily functions in thermoregulation. GTs occur most commonly in the subungual region of the finger, deep dermis, and subcutis of upper and lower extremities, but may rarely involve the mediastinum or viscera such as the stomach and lungs.
Microscopically, GTs are composed of three components: glomus cells, vasculature, and smooth muscle cells. Based on the relative proportion of these three components, GTs are divided into 3 different morphologic types: solid GTs (75%) are predominantly glomus cells, glomangiomas (20%) have a prominent vascular component, and glomangiomyomas (5%) contain prominent vasculature and smooth muscle components.
Typical GTs are benign and can be cured by complete surgical excision. Malignant GTs are exceedingly rare, comprising up to 2.9% of all GTs. Malignant GTs are characterized by atypical mitotic figures or marked nuclear atypia regardless of mitotic activity. Malignant GTs can be locally aggressive and one study showed 38% of malignant GTs metastasized. If a GT does not meet criteria for malignancy but has at least one atypical feature other than nuclear pleomorphism, it is categorized as GT of uncertain malignant potential. Symplastic GT is a variant with striking nuclear atypia in the absence of any other features indicative of malignancy.
Diagnosis of GT from a FNA specimen can be challenging because the aspirate may be hemorrhagic or paucicellular. The differential diagnosis varies based on the location, often including neuroendocrine tumor, paraganglioma, adnexal tumor in skin, and gastrointestinal stromal tumor in stomach, among others. GTs of all types typically express SMA and MSA. CD34 can be focally positive, but CD31 and ERG are negative in the glomus cells. GTs are negative for neuroendocrine tumor markers and melanocytic markers.
Question 3: Correct answer is CGT can be associated with syndromes like multiple familial glomus tumors and NF1. Sporadic benign and malignant GTs harbor recurrent NOTCH gene family rearrangements, with MIR143-NOTCH1/2/3 fusion genes in more than half of cases. BRAF mutation is detected in approximately 6% of GTs, all either malignant or of uncertain malignant potential.
REFERENCES:
- Mukherjee S, Bandyopadhyay G, Saha S, Choudhuri M, Cytodiagnosis of glomus tumor, J Cytol, 2010 Jul, PMID: 21187877
- Wood TR, McHugh JB, Siegel GW, Glomus tumors with malignant features of the extremities: a case series, Clinical Sarcoma Research, 2020 Oct
- Vidyavathi K, Udayakumar M, Prasad CS BR, Harendra K ML, Glomus tumor mimicking eccrine spiradenoma on fine needle aspiration, J Cytol, 2009 Jan-Mar, PMID: 21938152





