Case of the Month ...

A 73-year-old male with history of alcohol and tobacco use presented with abdominal pain, weight loss, and one episode of acute pancreatitis. MRI showed a hypodense lesion in the pancreatic head and EUS showed thickened duodenal folds with no intraluminal lesion, and an ill-defined hypoechoic and heterogeneous pancreatic head mass measuring 29 mm x 19 mm, with two enlarged peripancreatic lymph nodes. FNA of the pancreatic head lesion was performed.
Authors
- Daisy Sun, MD PhD, Miami Valley Hospital, Dayton, OH
- Mia Wang, The Seven Hills School, Cincinnati, OH
click on image for larger version
Figure 3 Figure 4 Images 1-4:
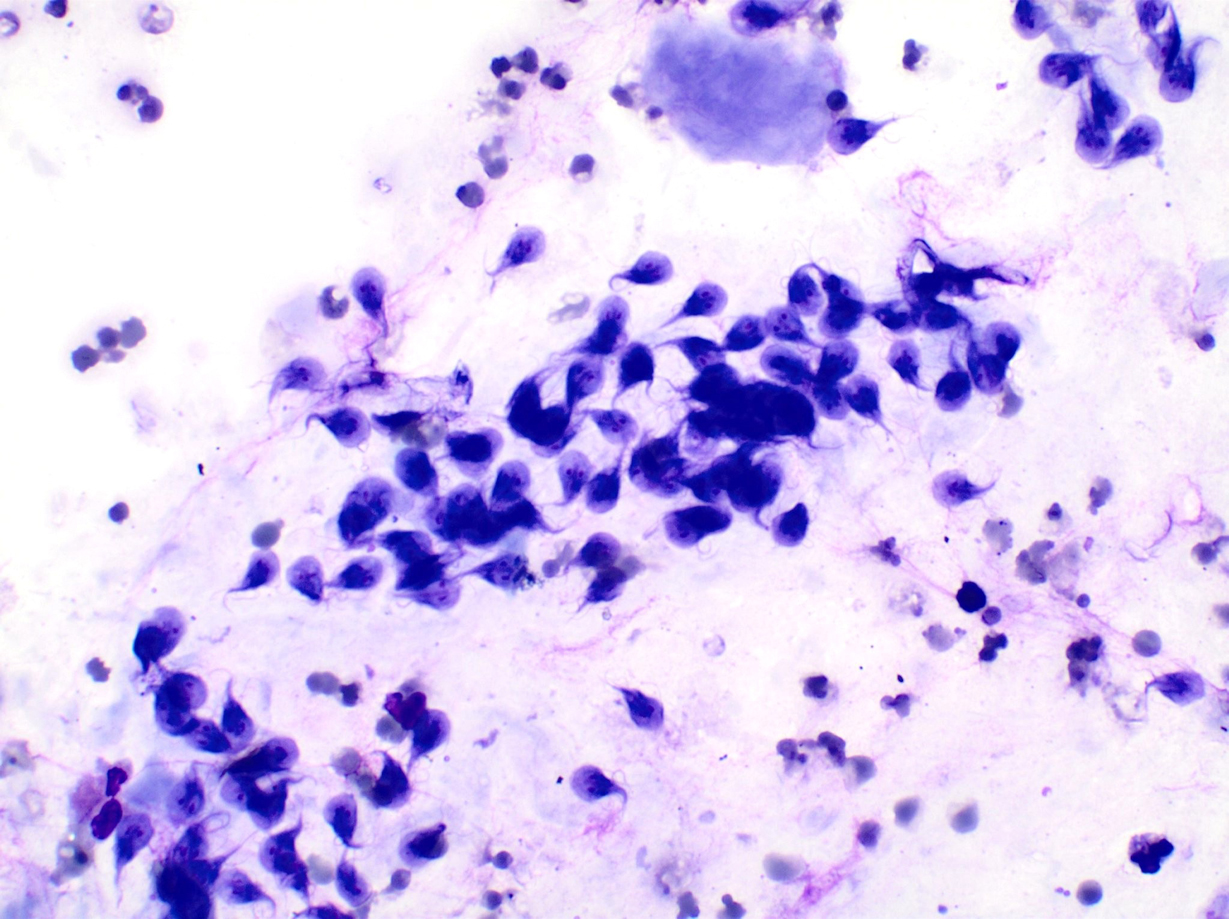
- Figure 1-2: Rapid on-site evaluation (ROSE) FNA material of pancreatic mass, smear, Diff-Quik stain, 40x magnification
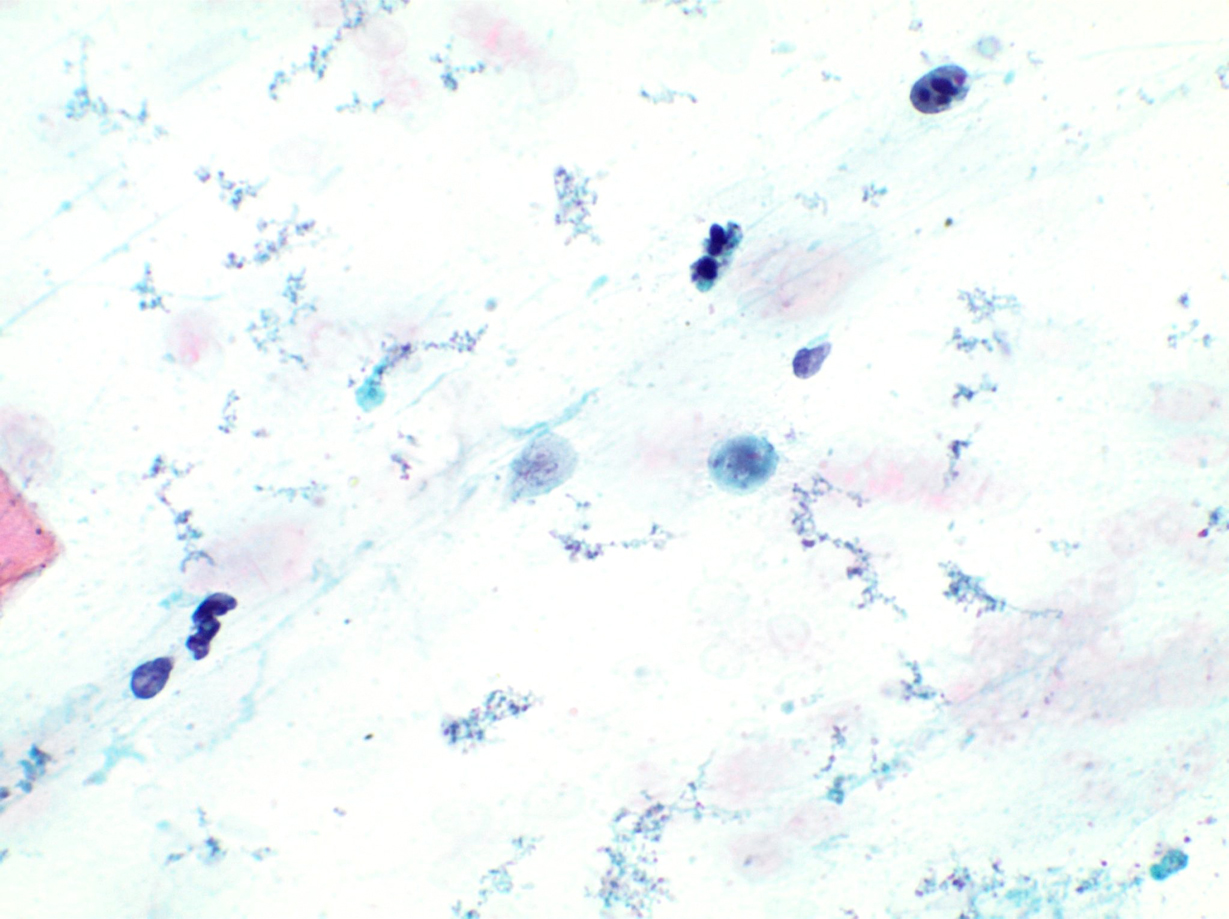
- Figure 3-4: Rapid on-site evaluation (ROSE) FNA material of pancreatic mass, smear, Pap stain, 40x magnification
Questions:
- What is the diagnosis?
- Giardiasis
- Amebiasis
- Strongyloidiasis
- Enterobius vermicularis egg
- Which of the following immunohistochemical or special stains can be used to identify Giardia?
- c-Kit (CD117)
- DOG 1
- AFB
- PAS
Answers:
Question 1: Correct answer is A
The smears (Figure 1-4) show inflammatory cells and reactive epithelial cells that are not diagnostic of carcinoma. Strikingly, there are numerus microorganisms consistent with trophozoites of Giardia duodenalis displaying characteristic pear-shaped, binucleated, flagellated morphology.Giardia duodenalis was first described by van Leeuwenhoek in 1681 while he was examining his own diarrheal stool. Giardiasis is the most common waterborne parasitic infection of GI tract worldwide. Its prevalence ranges from 2-7% in developed countries to 20-30% in developing countries. Clinical presentation varies from asymptomatic to diarrhea, weight loss, abdominal pain, or chronic malabsorption, depending on many factors including the state of the host immune system, host age, host nutritional status, and strain genotype, amongst others.
Giardia. duodenalis infects the small intestine and colonizes the epithelial surface and lumen. Extraintestinal manifestations are not entirely uncommon. It has been reported that Giardia. duodenalis exists in pancreas, stomach, cecum, or distal small intestine. Coincidence of Giardiasis with pancreatitis or pancreatic tumor has been described.
The life cycle of Giardia. duodenalis consists of two stages: trophozoites and cysts. The G. duodenalis cyst is environmentally stable. After ingestion, the cyst passes through the acidic stomach into the duodenum where excystation occurs upon exposure to bile and a more alkaline pH environment. The trophozoite is the vegetative form and replicates in the small intestine of the host. The trophozoite encysts into a cyst in the distal small bowel or colorectum and is passed in the stool, allowing for transmission to the next host through a fecal-oral route. The G. duodenalis trophozoite is pear-shaped, with a length of 12 to 15 um and a width of approximately 8 um. It has 4 pairs of flagella, providing motility, and a concave ventral side allowing the organism to attach to the intestinal epithelium for nutritional absorption. The dorsal surface is convex, and two symmetrical nuclei are in the anterior half.
Question 2: Correct answer is A
The diagnosis can be established by microscopic examination of a fecal sample, immunologic detection of stool antigens, PCR, and others. Endoscopic biopsy and examination of duodenal contents is an alternate method to identify trophozoites, with the potential of identifying other etiologies. Duodenal biopsy can have a wide range of histological features, ranging from normal villous architecture to variable villous blunting and increased inflammatory cells. Demonstration of G. duodenalis is the key for diagnosis. These parasites have a “falling leaves” appearance on routine light microscopy, floating freely in the lumen between duodenal villi, adherent to the mucosal surface but not invading it. G. duodenalis can be inconspicuous on routine H&E stain, and can still be missed even with special stains such as Giemsa or trichrome. c-Kit (CD117) immunohistochemistry has been described to create a specific appearance by accentuating its paired nuclei and function as a sensitive immunohistochemical method to detect G. duodenalis.REFERENCES:
Igor Sinelnokov, Netta Sion-Vardy, Ruthy Shaco-Levy, c-kit(CD117) immunostain is useful for the diagnosis of Giardia lamblia in duodenal biopsies, Human Pathology, March 2009
- Marie CM Halliez, Andre G Buret, Extra-intestinal and long-term consequences of Giardia duodenalis infections, World Journal of Gastroenterology, 2013
- Rodney D Adam, Giardia duodenalis: Biology and Pathogenesis, Eukaryotic Cells, 2021