Case of the Month ...
A 54-year-old male with no significant past medical history presented to the Emergency Department with shortness of breath, chest pain and severe hypotension. CT chest revealed a large pericardial effusion concerning for tamponade, multiple bilateral pulmonary masses with surrounding ground glass opacities, and a small right pleural effusion. Cytology evaluation of the sanguinous pericardial fluid was negative for malignancy. Transesophageal Echocardiogram showed a friable right atrial mass with broad based attachment to the lateral wall. The largest lung mass (3 cm) was on the right, in aparamediastinal and anterior location. Fine needle aspiration (FNA) of this lung mass was performed.
Authors
- Daisy Sun, MD PhD, Miami Valley Hospital, Dayton, OH
- Mia Wang, The Seven Hills School, Cincinnati, OH
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
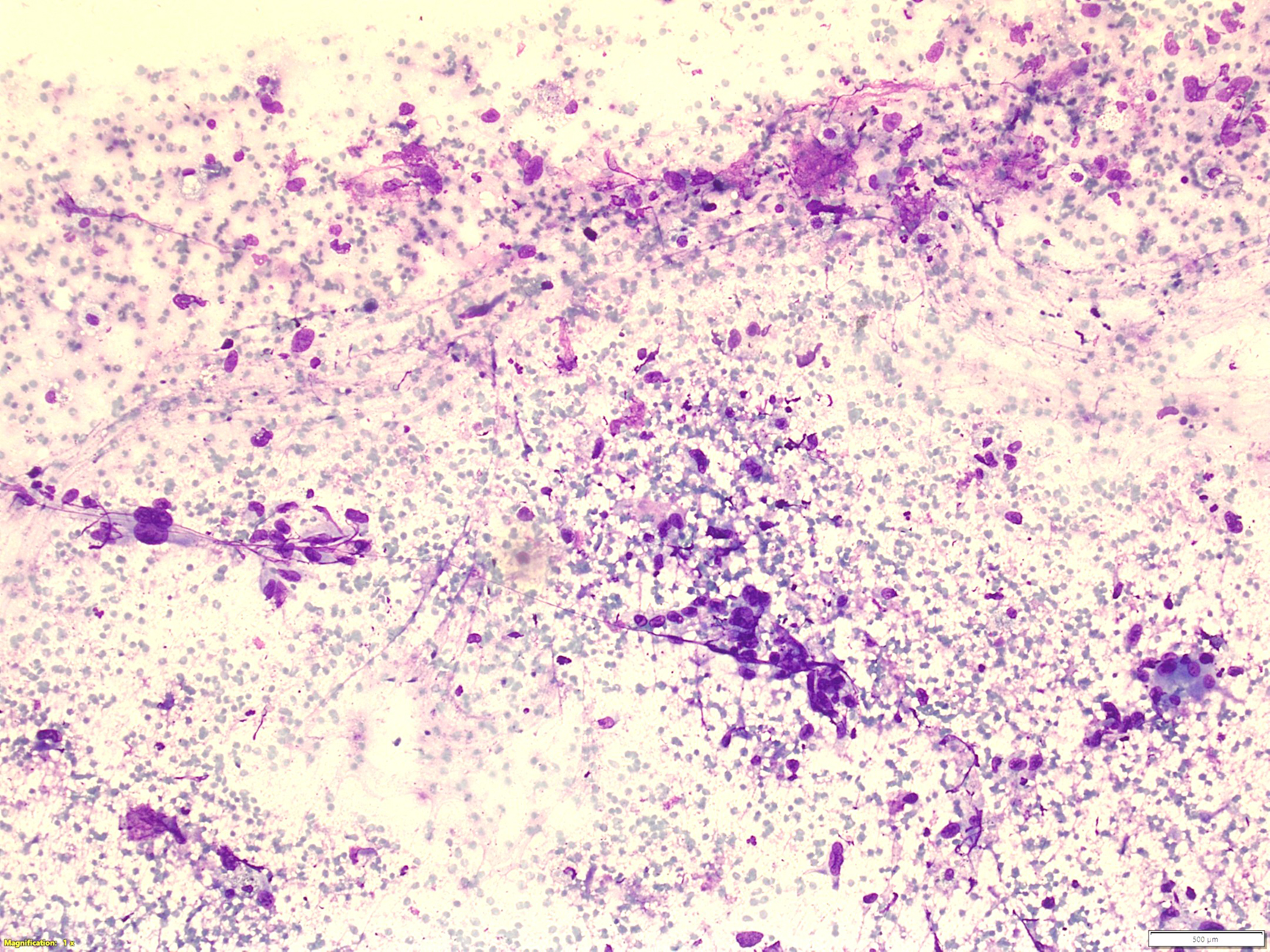
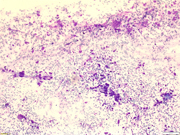
- Figure 1: Rapid on-site evaluation (ROSE) FNA material of right lung mass, smear, Diff-Quik stain, 40x magnification.
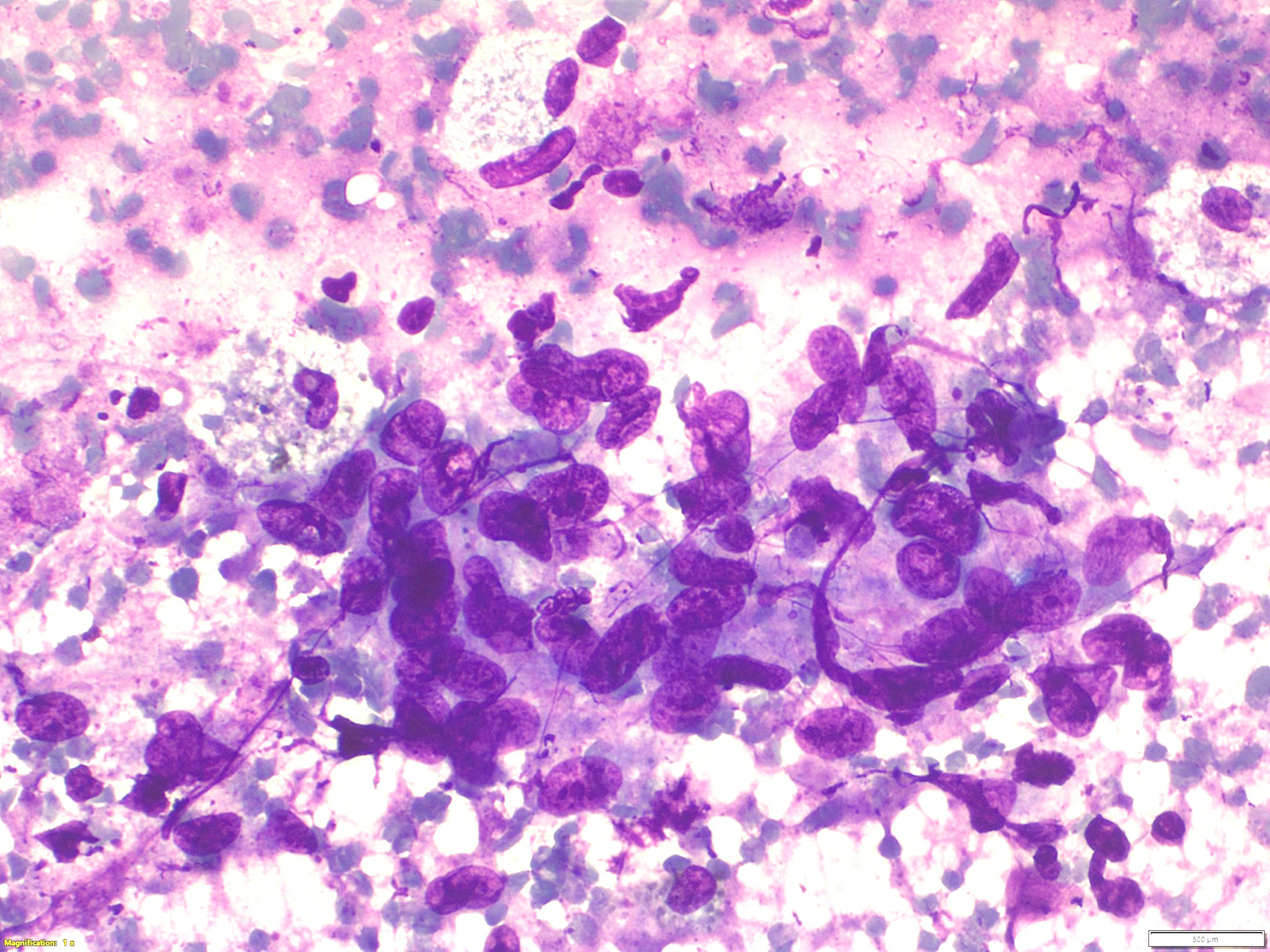
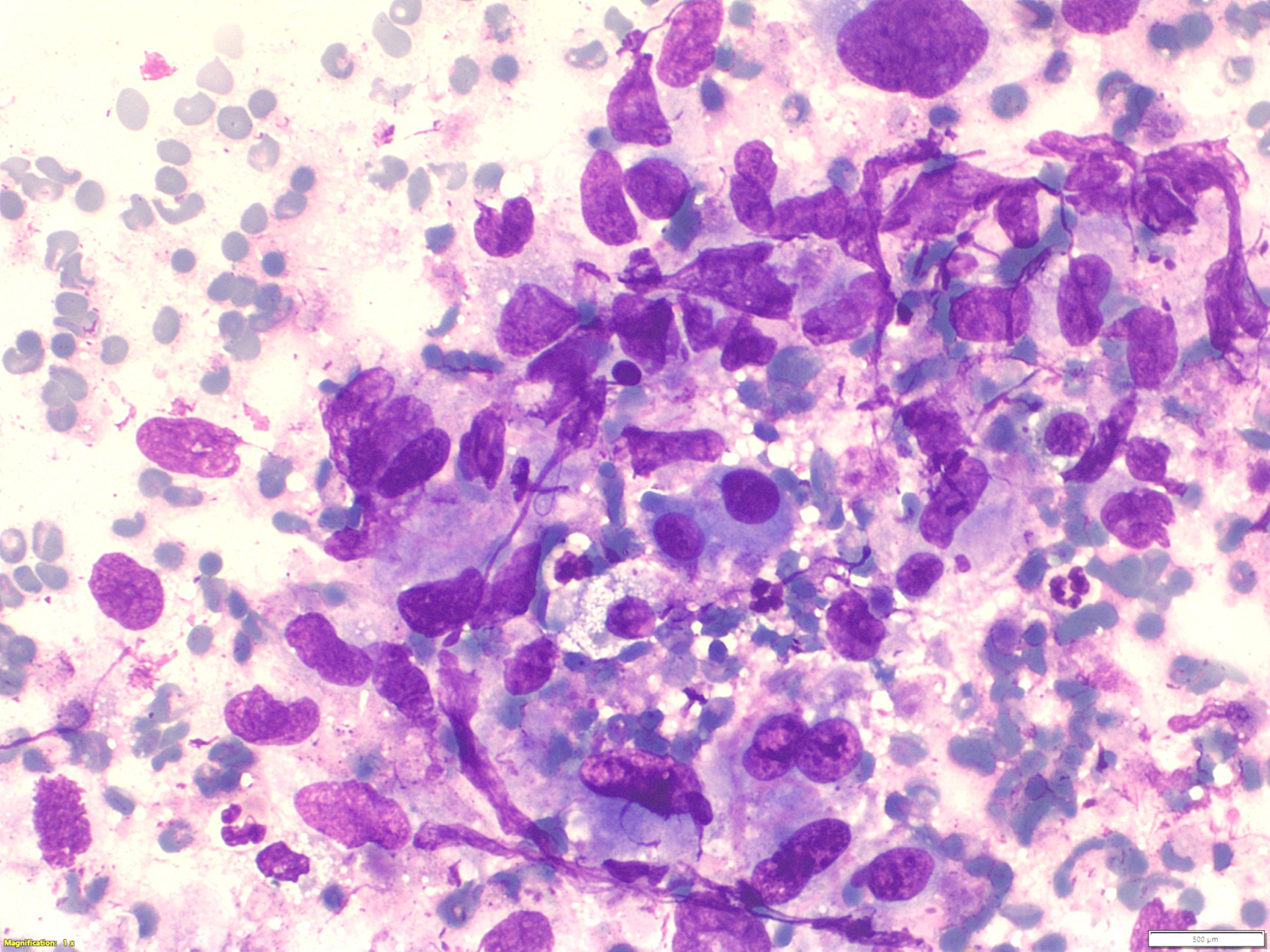
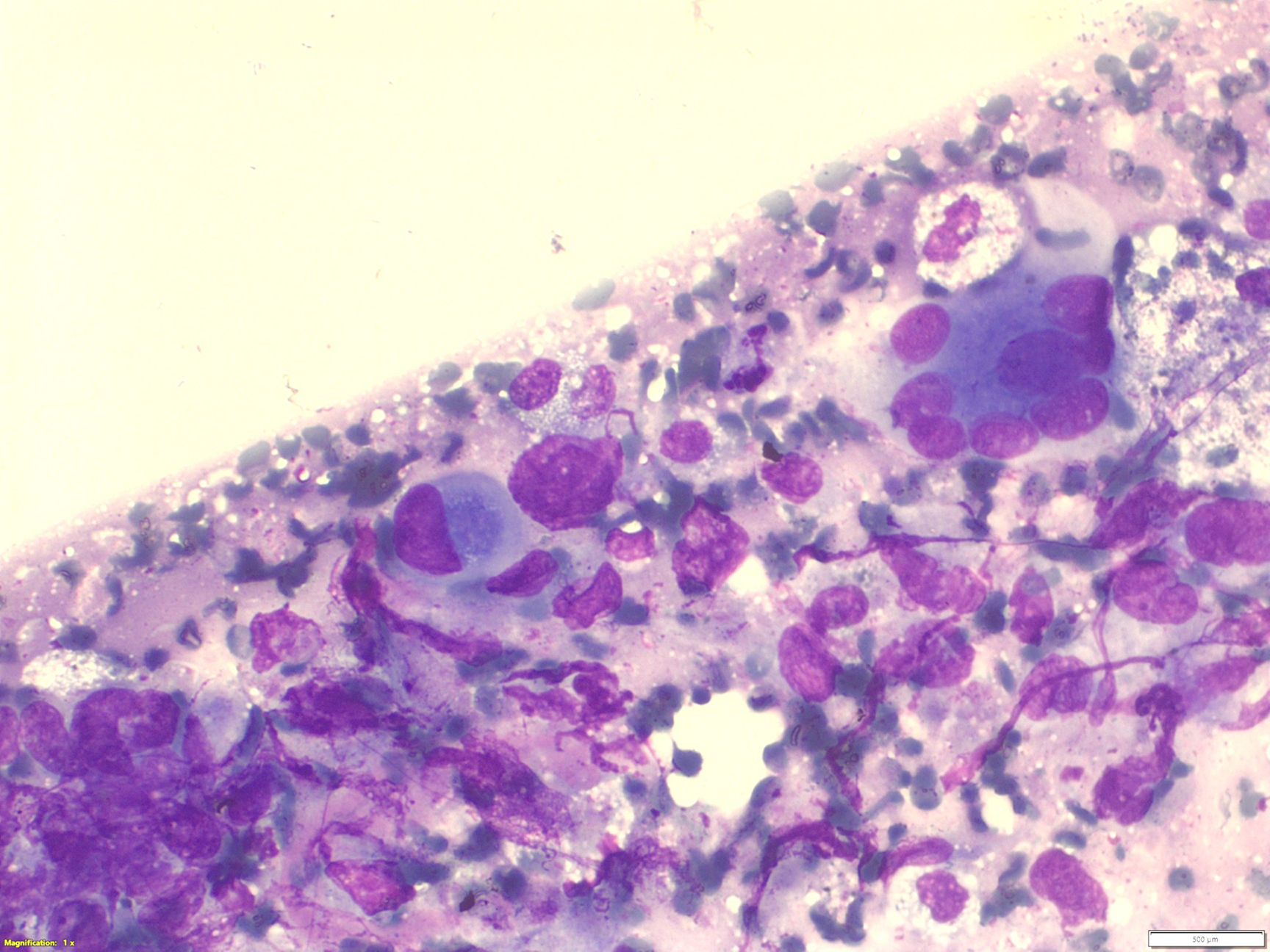
- Figure 2-4: Rapid on-site evaluation (ROSE) FNA material of right lung mass, smear, Diff-Quik stain, 400x magnification.
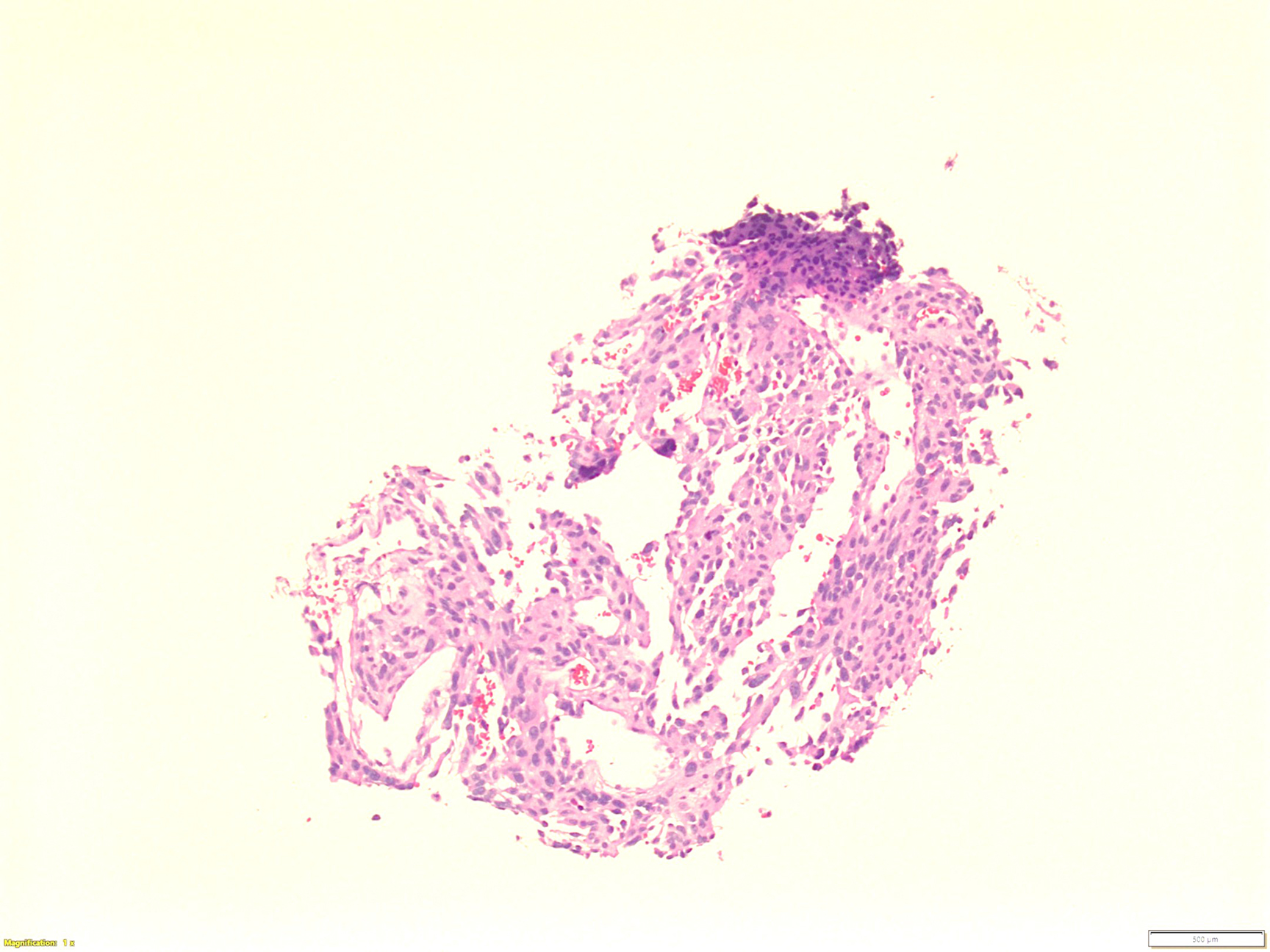
- Figure 5: Right lung mass, core biopsy, H&E stain, 100x magnification.
- Figure 6: Right lung mass, core biopsy, ERG immunohistochemistry, 100x magnification
Questions:
- What is the diagnosis?
- Angiosarcoma
- Granulomas
- Poorly differentiated carcinoma
- Metastatic melanoma
- Which of the following immunohistochemical stain is most likely positive in angiosarcoma?
- FOS
- CAMTA1
- HHV 8
- ERG
- SOX 10
Answers:
Question 1: Correct answer is A
The aspiration (Figure 1) is cellular and composed of atypical cells singly dispersed or loosely clustered. High power images (Figure 2-3) demonstrate tumor cells, both spindled and epithelioid, displaying marked enlarged and irregular nuclei with prominent nucleoli. Figure 4 depicts cells wrapping around each other and a multinucleated giant cell nearby. The FNA was aborted due to bleeding and the minute core biopsy appears vascular and hemorrhagic. Immunohistochemistry performed on the core biopsy shows that these cells of interest are strongly and diffusely positive for ERG, while negative for AE1/3, TTF-1, p40, and S100. Ki-67 is increased and p53 is overexpressed. A metastatic angiosarcoma (AS) from the right atrium is rendered.
Primary cardiac tumors are very rare and 20-30% of all primary cardiac tumors are malignant, including AS, lymphoma, fibrosarcoma, myosarcoma, and myxosarcoma. AS is the most common cardiac malignancy in adults, accounting for 25-30% of the cases. Cardiac AS arises from the endothelial cells and is considered the most fatal and aggressive primary cardiac malignancy, due to its rapid local infiltration and growth, high rate of systemic metastasis, poor response to adjuvant therapy, lack of targeted therapy, and other factors. About 90% of cardiac AS are located in the right atrium, followed by left atrium, then right and left ventricles. The most common metastatic site is the lung, followed by the liver, brain, bone, lymph nodes, pancreas, spleen, adrenal gland, and kidney.
The most common clinical presentation includes chest pain, myalgia, palpitations, and commonly associatedpericardial effusions, cardiac tamponade, and heart failure. Hemorrhagic pericardial fluid strongly indicates a malignant nature of the process and a diagnosis of AS can be made on a fluid specimen; however, the diagnostic value of a fluid specimen is very limited, as shown in our case, and a tissue sample is necessary.Question 2: Correct answer is D
Cytological findings from an FNA of AS can be variable, with a wide range of cytomorphologic characteristics. Previously described cytological features include increased cellularity, spindled or epithelioid cells, prominent nucleoli with club-shaped/bar-like nucleoli, chromatin stranding, atypical mitosis, and vasoformative features including hemophagocytosis, intracytoplasmic lumina and lumina containing red blood cells or neutrophils, and endothelial wrapping. Club-shaped/bar-like nucleoli by definition was at least 3 times as long or as wide as normal nucleoli and are elongated at one end. Chromatin stranding was described as thin extensions connecting the nucleolus to the nuclear membrane. Despite search for these features in this aspiration specimen, only one focal vague endothelial wrapping is identified.
The differential diagnosis of AS includes melanoma, poorly differentiated carcinoma, when AS demonstrates a predominantly epithelioid appearance, plasmacytoma, and other vascular lesions including epithelioid and spindle cell hemangioma (EH), epithelioid hemangioendothelioma (EHE), and Kaposi’s sarcoma (KS). AS expresses vascular markers including ERG, CD31, CD34, and D2-40. It is negative for CD138, HHV8, and melanoma markers. Epithelial markers can be positive if the lesion has an epithelioid component. KS is a low-grade vascular tumor associated with HHV-8 infection and is one of the most common neoplasms reported in AIDS patients. HHV-8 is the most diagnostically specific immunostain to differentiate KS from other vascular lesions. Differentiation between EH and EHE vs. AS is vital, yet challenging, due to significant cytological, immunohistochemical, and clinical overlapping. More recent focus in molecular diagnosis has identified recurrent WWTR1-CAMTA1 or YAP1-TFE3 gene fusion in EHE and FOS rearrangement in EH. An accurate diagnosis of AS relies on meticulous evaluation of the cytomorphology, clinical and radiological correlation, and judicious use of ancillary immunohistochemical and molecular analysis.REFERENCES:
- Rachel L Geller, Kim Hookim, Harold C Sullivan, Lauren N Stuart, Mark A Edgar, Michelle D Reid , Cytologic features of angiosarcoma: A review of 26 cases diagnosed on FNA, Cancer Cytopathol, 2016
- Karen Thomas MD, Haley Trinh, Anna Fei, Laila Khazai MD, Hongxia Sun MD, PhD, Qiong (Jenny) Gan MD, PhD, Cytologic features of angiosarcoma in fluid specimens: A retrospective study of 22 cases. Cancer Cytopathol, 2025
- Yujian Guo, Qianzhen Liu, Haibo Wu, Primary cardiac tumor: a case report of right atrial angiosarcoma and review of the literature, Front Oncol, 2023