Case of the Month ...
A 65-year-old male patient presented to the Emergency Department (ED) with chest, abdominal, and back pain which had been ongoing for a few weeks. He denied shortness of breath, nausea, vomiting, and weight loss. He had a significant history of smoking and drinking, and denied a prior history of cancer. Abdominal CT showed a soft tissue density in the pancreatic tail described as a 3.4 x 2.3 cm mass, along with multiple lung lesions, concerning for possible pancreatic adenocarcinoma with lung metastasis. Endoscopic Ultrasound-Guided Fine-Needle Aspiration (EUS-FNA) with Rapid on Site Evaluation (ROSE) of the pancreatic tail mass was performed.
Authors
- Daisy Sun, MD PhD, Miami Valley Hospital, Dayton, OH
- Mia Wang, The Seven Hills School, Cincinnati, OH
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6
Figure 1-6:
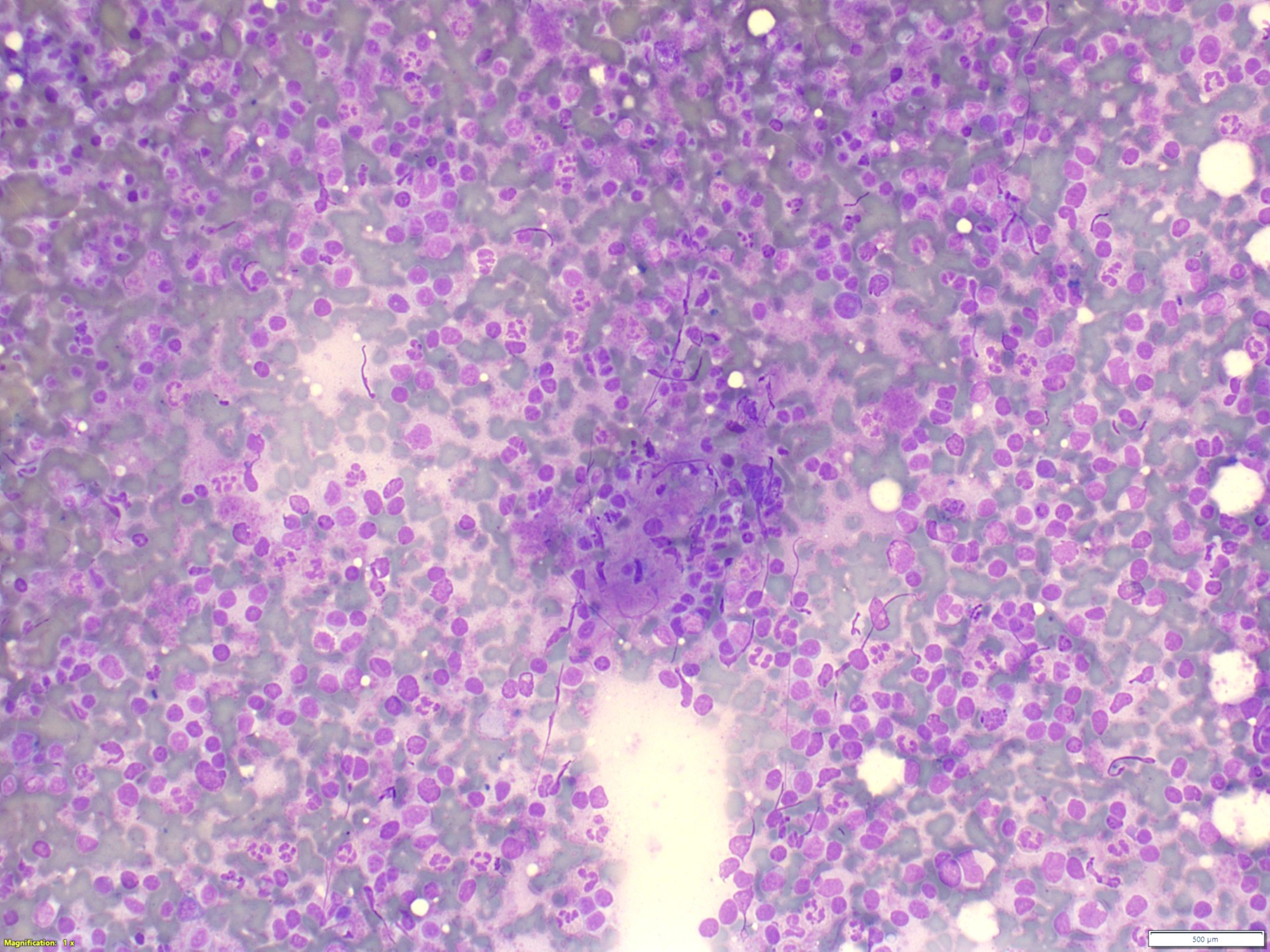
- Figure 1: Rapid on-site evaluation (ROSE) FNA material of pancreatic tail mass, smear, Diff-Quik stain, 40x magnification.
- Figure 2: Rapid on-site evaluation (ROSE) FNA material of pancreatic tail mass, smear, Diff-Quik stain, 100x magnification.
- Figure 3: Rapid on-site evaluation (ROSE) FNA material of pancreatic tail mass, smear, Diff-Quik stain, 200x magnification.
- Figure 4: Rapid on-site evaluation (ROSE) FNA material of pancreatic tail mass, smear, Pap stain, 200x magnification.
- Figure 5: Pancreatic tail mass, core biopsy, 100x magnification.
- Figure 6: Pancreatic tail mass, core biopsy, CD8 immunohistochemistry, 100x magnification.
Questions:
- What is the diagnosis?
- Well-differentiated pancreatic neuroendocrine tumor
- Chronic inflammation
- Intrapancreatic accessory spleen
- Low grade lymphoma, NOS
- Which of the following statements about accessory spleen is correct?
- The most common location of AS is pancreatic tail
- An AS has distinctive histology
- AS does not require surgical treatment after splenectomy in patient with autoimmune hemolytic anemia
- CD8 is a specific marker for splenic venules
Answers:
Question 1: Correct answer is C
The smears (Fig. 1-3) are cellular containing mostly dyscohesive cells with rare tissue fragments. Higher power demonstrates dispersed polymorphous lymphocytes that are predominantly small mature lymphocytes admixed with neutrophils, histiocytes, and eosinophils. The pap smear (Fig. 4) shows tissue fragments composed of small blood vessels surrounded by abundant lymphocytes. No epithelial cells are identified. The cell block and core biopsy are bloody, displaying small slit-like vascular spaces surrounded by lymphocytes, eosinophils, and plasma cells. Immunostain for CD8 highlights and confirms the presence of splenic sinusoidal endothelial cells. of the correct diagnosis is intrapancreatic accessory spleen (IPAS).
Question 2: Correct answer is D
The spleen is a large encapsulated organ, composed of vascular and lymphatic tissue. The spleen is derived from splanchnic mesoderm during the 5th week of embryogenesis. Initially, the developing spleen is closely associated with the developing dorsal pancreas, and its mesenchyme shares common origin with the mesenchymal parts of the developing pancreas. Between the 6th and 7th week, the spleen is translocated to the left side of the abdominal cavity, which is very close to the developing gonad and epididymis, due to the rotation of the stomach. The developing spleen continues to grow and separate from the dorsal mesogastrium. Finally, the spleen is anchored in the left upper abdomen and connects to the stomach via the gastrosplenic ligament and to the left kidney and posterior body wall via the splenorenal ligament.
Ectopic splenic tissue (EST) is the presence of functional splenic tissue outside of its normal anatomical position, either due to an error during development (congenital) or fragmentation of the spleen causing seeding and implantation (acquired).
Various congenital anomalies, developmental defects, or anatomical variations of the spleen have been described, including accessory spleen (AS), wandering spleen, lobulation of spleen, splenogonadal fusion, etc. AS is a congenital anomaly due to incomplete migration and fusion of splenic primordia during embryogenesis. AS is often located in splenic hilum (62-80%), followed by near the pancreatic tail (16%). It also can occur anywhere in the abdomen, including the gastric wall, colon, omentum, mesentery, and even the scrotum. AS is usually single (74-85%), but two or more have been observed. Grossly, AS appears as a solid mass and histologically and functionally AS is similar to normal spleen.
Splenosis is an acquired type of EST. Splenosis is defined as an autotransplantation of the splenic tissue in a heterotopic location that primarily develops after splenic trauma or surgery. Splenic fragments after trauma or surgery can seed onto vascularized intra- or extraperitoneal surfaces, usually in abdominopelvic cavity, but it also described in intrathoracic, subcutaneous, intrahepatic, or intracranial tissues.
When EST presents as an intrapancreatic lesion, FNA is commonly used for pre-surgical evaluation. Radiologically, intrapancreatic AS (IPAS) usually appears as a well-defined solid lesion; however, it can undergo spontaneous hemorrhage with subsequent cystic degeneration. The cytological findings associated with IPAS are not specific and are composed of a mixture of lymphoid cells, neutrophils, eosinophils and red blood cells. Scattered transversing small blood vessels might be seen. The differential diagnosis, based on the imaging and cytological findings, includes well-differentiated neuroendocrine tumor (PanNET), solid pseudopapillary neoplasm (SPN), pancreatic ductal adenocarcinoma, lymphoepithelial cyst, chronic pancreatitis, hemangioma, benign peripancreatic lymph node, and even lymphoma. Ancillary studies, including immunohistochemistry and flow cytometry help establish a definite diagnosis. CD8 is a key immunohistochemical marker to confirm splenic tissue. CD8 specifically highlights splenic venules, separating IPAS from a lymph node and other vascular anomalies. AE1/3 fails to reveal an epithelial component, ruling out carcinoma.
EST is a benign anatomical variation that is either congenital or acquired. It is typically asymptomatic, discovered incidentally, with slow growth, and requires no surgical intervention unless complications, such as torsion or rupture with hemorrhage, occur. Though mostly discovered incidentally for unrelated reasons, EST can cause imaging enigmas and become a diagnostic challenge. EST in the gastric wall may be mistaken for an enlarged lymph node. Abdominal or pelvic splenosis is generally multifocal, simulating widely spread metastatic disease. Atypical and unusual locations of EST such within the pancreas, kidney, liver, and brain, are clinically concerning and may also be diagnostically challenging. Despite being a benign process, EST could be important in the setting of therapeutic splenectomy for hematopoietic diseases. EST might undergo compensatory hypertrophy after splenectomy, causing relapse of disease. It is thus recommended to search for ESTs and perform ectopic splenectomy in such patients.
FNA of our patient’s pancreatic lesion revealed a benign IPAS and subsequent lung biopsy demonstrated lung adenocarcinoma.
REFERENCES:
- Alexander Mayer, Ivan Varga, David Kachlik, Jaroslav Voller, Ivan Fuljer, Peter Jackuliak. Accessory Spleen: An Anatomical Variation or Developmental Defect? Surgical, Anatomical and Embryological Perspectives. Bratislava Medical Journal, 2025.
- Mine Islimye Taskin, Banu Guleç Baser, Ertan Adali, Erdoğan Bulbul, Engin Uzgoren. Accessory spleen in the pelvis: A case report. Int J Surg Case Rep, 2015.
- Emily W Gripp, Stacey M Gargano. “Sneaky Spleen”: Three Cases of Ectopic Splenic Tissue Mimicking Neoplasia. Case Rep Pathol, 2025.