Case of the Month ...
A 16-year-old female presented with abdominal distention, intermittent epigastric pain, early satiety, and weight loss. Magnetic resonance imaging of abdomen and pelvis revealed a solid pancreatic head mass, measuring 3.8 x 2.8 x 2.1 cm. Trans-duodenal endoscopic ultrasound-guided fine-needle aspiration biopsy from the head of the pancreas was successfully performed.
Authors
- Yodsuí Figueroa Hernández, MD. Cytopathology Fellow. Department of Pathology and Cell Biology. Columbia University Irving Medical Center. New York Presbyterian Hospital, New York, NY
- Rachelle P. Mendoza, MD. Assistant Professor of Pathology and Cell Biology. Department of Pathology and Cell Biology. Columbia University Irving Medical Center. New York Presbyterian Hospital, New York, NY
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
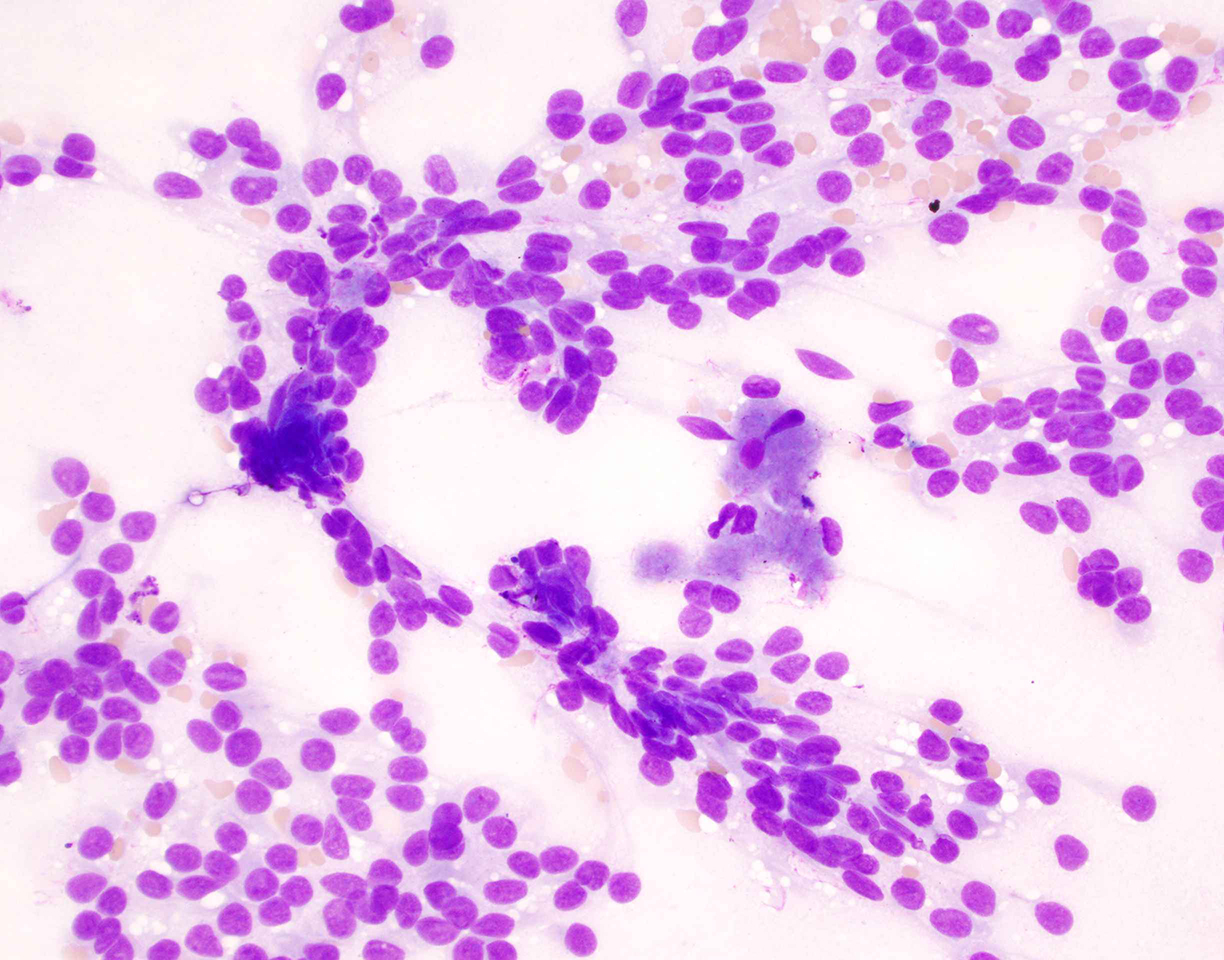
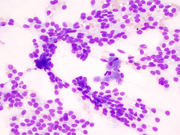
- Figure 1: FNA material, smear, Diff-Quick stain, 40x magnification
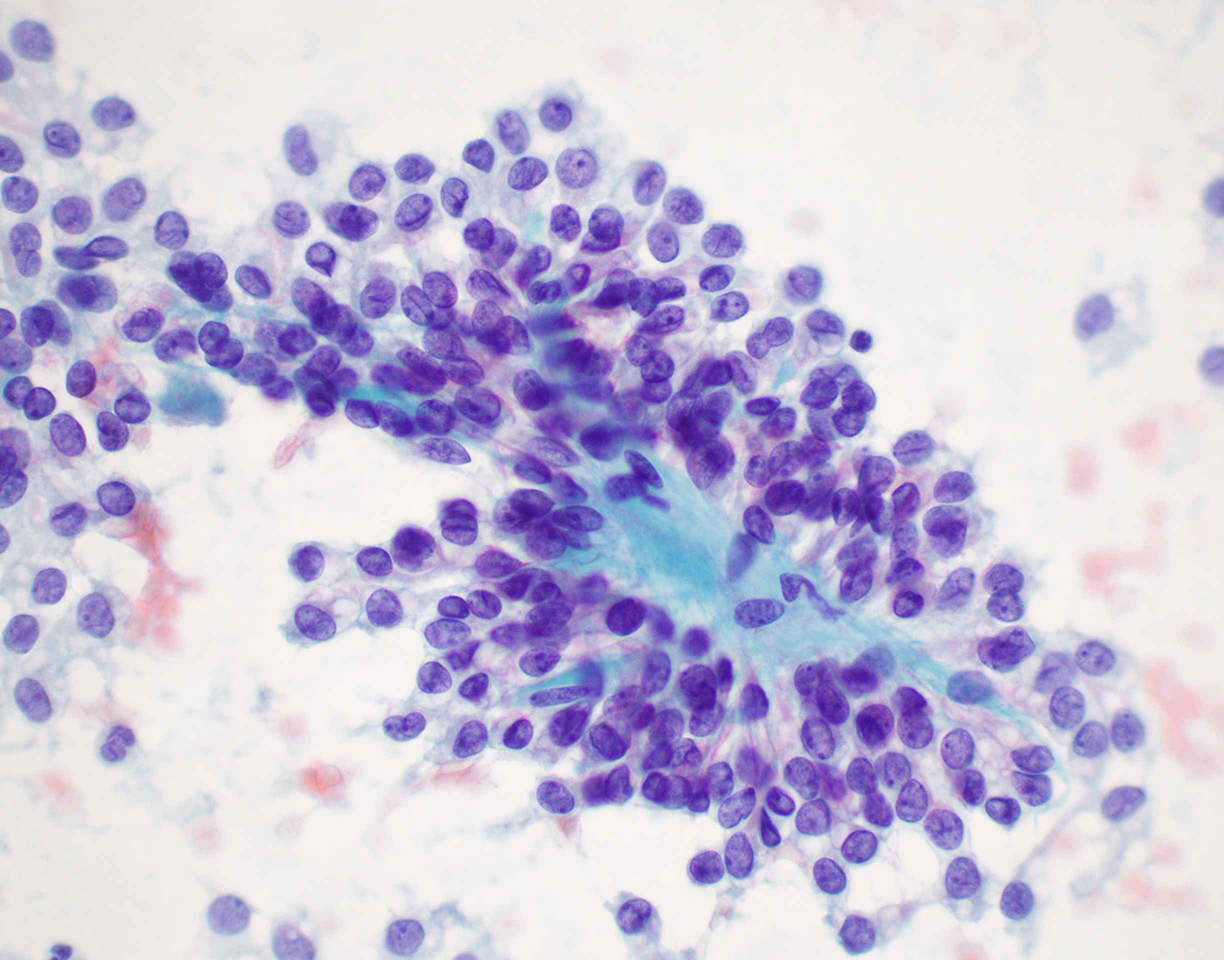
- Figure 2: FNA material, smear, Pap stain, 60x magnification
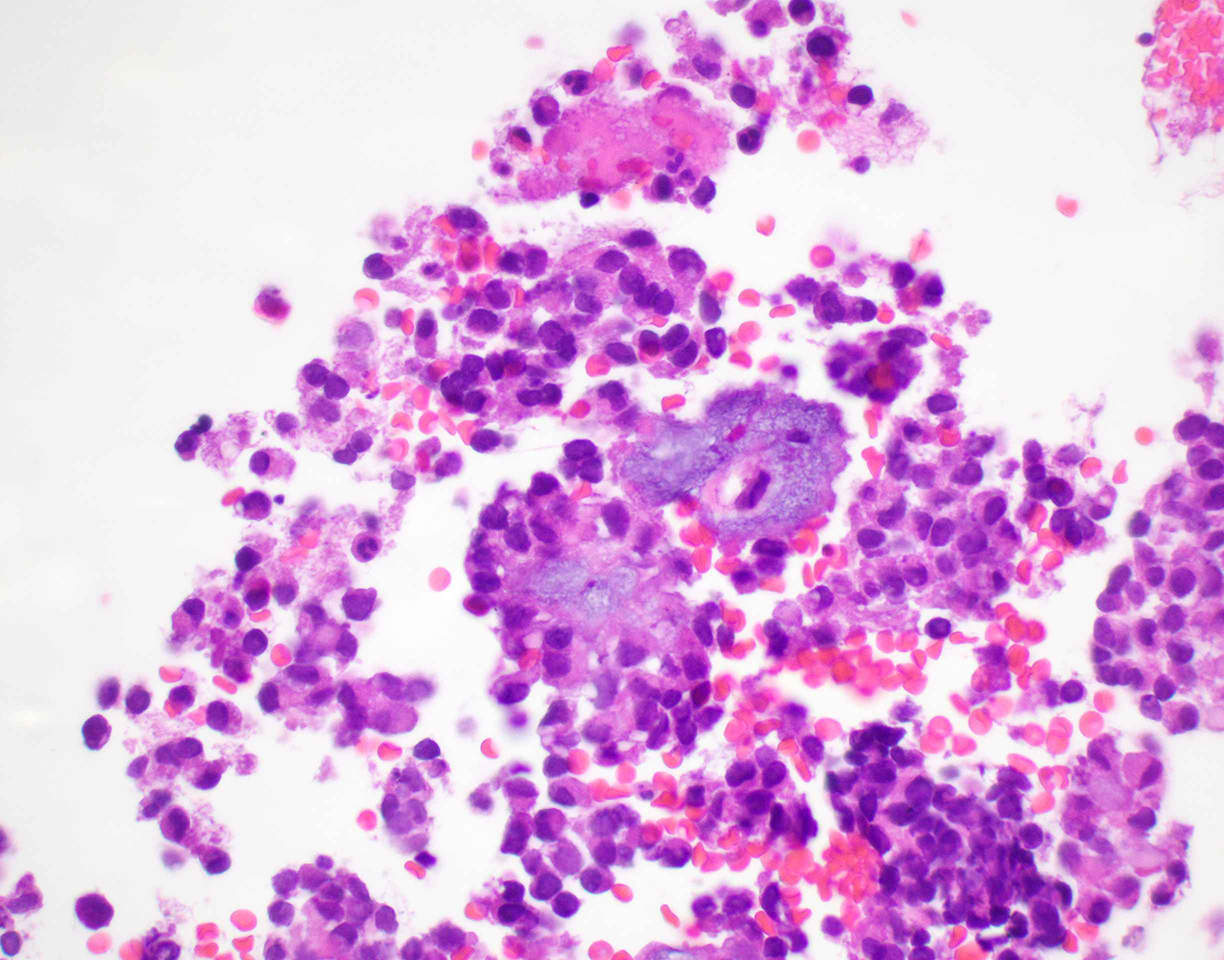
- Figure 3: Cell-block, H&E stain, 60x magnification
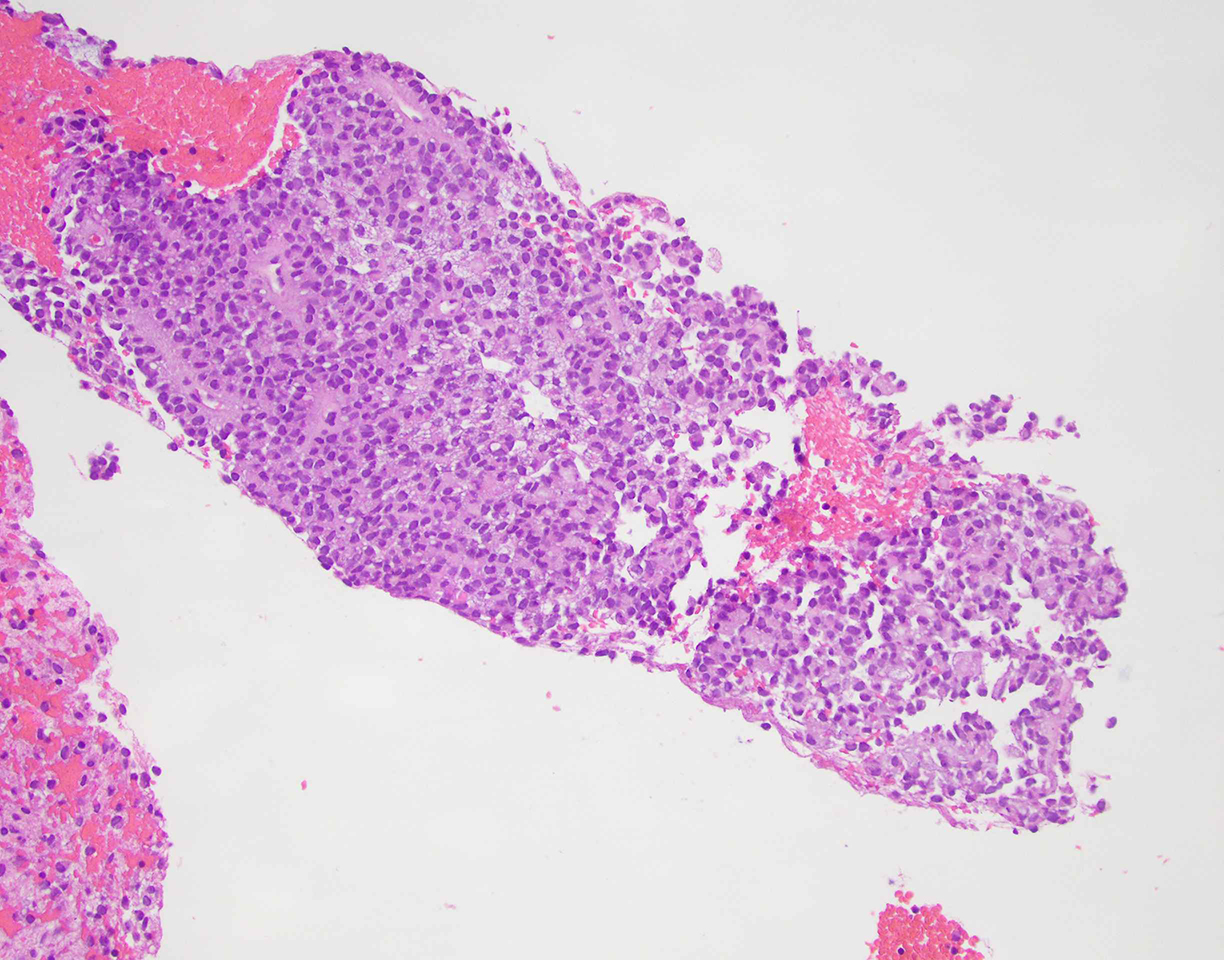
- Figure 4: Cell-block, H&E stain, 20x magnification
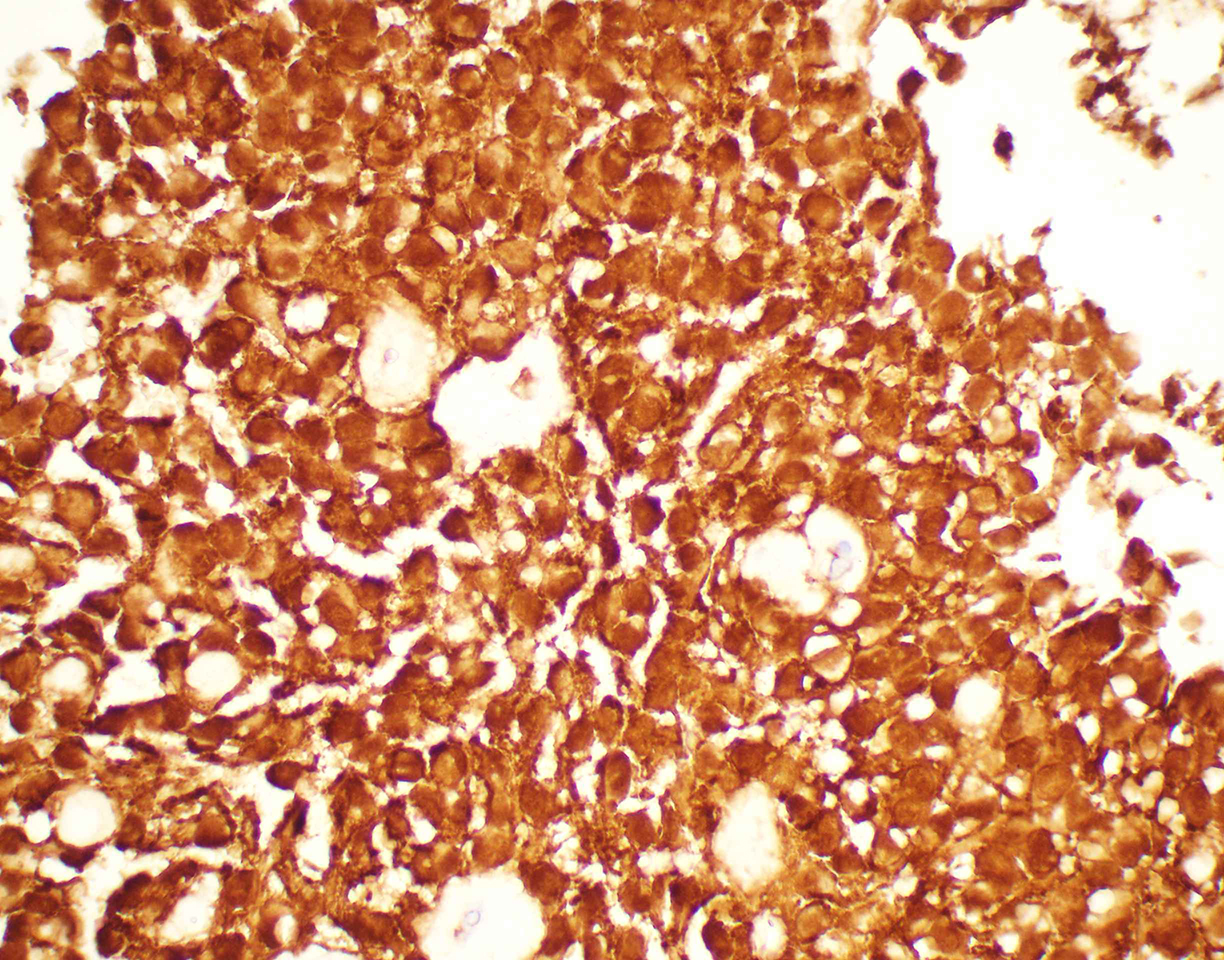
- Figure 5: Cell-block, Beta-catenin immunohistochemical stain,60x magnification
- Figure 6: Cell-block, E-cadherin immunohistochemical stain, 20x magnification
Questions:
- What is the best diagnosis based on the clinical presentation, cytomorphology, microbiopsy architecture and immunohistochemical findings?
- Pancreatoblastoma
- Acinar cell carcinoma (ACC)
- Pancreatic neuroendocrine tumor (PanNET)
- Metastatic ovarian carcinoma
- Solid pseudopapillary neoplasm (SPN)
- Which diagnostic category does this tumor correspond to in the World Health Organization (WHO) Reporting System for Pancreatobiliary Cytopathology?
- Benign, non-neoplastic
- Benign, neoplastic
- Malignant
- Pancreatobiliary neoplasm, high-risk/grade
- Pancreatobiliary neoplasm, low-risk/grade
- What is the genetic mutation most commonly seen in this tumor?
- CTNNB1 (β-catenin pathway)
- GNAS
- p53
- VHL
- KRAS
- Which of the following markers is positive in the metachromatic hyaline globules present within this tumor?
- Congo red
- α1-Antitrypsin
- CD56
- CPA1/2
- Trypsin
Answers:
Question 1: Correct answer is E.Solid pseudopapillary neoplasm (SPN)
SPN is a low-grade malignant pancreatic tumor composed of poorly cohesive epithelioid to plasmacytoid cells forming solid and pseudopapillary structures. The definitive cell of origin remains unclear. These tumor cells appear bland and uniform with a moderate amount of cytoplasm, which contains clear perinuclear vacuoles and/or hyaline globules. Nuclei are round to oval with grooves and finely granular chromatin.
Both PanNET and ACC may also be composed of relatively bland epithelioid to plasmacytoid cells that are loosely cohesive. PanNET typically will demonstrate a finely stippled (salt and pepper) nuclear chromatin, whereas ACC typically demonstrates conspicuous nucleoli and a distinctly granular cytoplasm. All three tumors commonly demonstrate stripped naked nuclei due to the fragility of the lesional cells. PanNET are typically cytokeratin positive, as well as diffusely positive for neuroendocrine markers (synaptophysin, chromogranin, INSM1). ACC are also cytokeratin positive tumors that can show focal staining with neuroendocrine markers, particularly synaptophysin; however, these tumors will demonstrate cytoplasmic positivity for markers of acinar differentiation, specifically trypsin and chymotrypsin. Other markers that can be helpful in ACC include BCL10. LEF1 immunohistochemistry can be utilized as a diagnostic marker in SPN, though a minority (<20%) of ACC may also be LEF1 positive and/or show nuclear localization of beta-catenin.
The cytomorphology of pancreatoblastoma typically resembles a small round blue cell tumor with cytomorphologic features that overlap with entities such as small cell carcinoma. A unique feature of pancreatoblastoma are the presence of squamoid morules, which show nuclear locatlization of beta-catenin, and are extremely helpful in rendered a correct diagnosis if observed.
Question 2: Correct answer is C. Malignant
The World Health Organization (WHO) Reporting System for Pancreatobiliary Cytopathology in conjunction with the International Academy of Cytology and the International Agency for Research on Cancer standardized a system for reporting pancreatobiliary cytopathology. This system subdivided diagnoses into seven diagnostic categories (Non-Diagnostic, Benign, Atypical, PaN-Low, PaN-High, Suspicious for Malignancy, Malignant), a distinct departure from the six-tiered system of the predecessor framework, the Papanicolaou Society of Cytopathology System for Reporting Pancreatobiliary Cytopathology (Non-Diagnostic, Negative, Atypical, Neoplastic, Suspicious for Malignancy, Malignant).
Question 3: Correct answer is A. CTNNB1
Point mutation in exon 3 of β-catenin gene (CTNNB1) is present in > 90% of SPNs. This genetic mutation results in the accumulation of β catenin in the cytoplasm and formation of a β-catenin Tcf/Lef complex, through which the WNT signaling pathway activates several oncogenic genes, such as MYC and cyclin D1. Rarely, mutations in the APC gene have been described.
Question 4: Correct answer is B. α1-Antitrypsin
The intracytoplasmic hyaline globules of SPN are PAS positive, diastase-resistant, and immunoreactive with α1-Antitrypsin.
References
- Granados, R; Stelow, E. B; Centeno, B. A. WHO Classification of Tumours. WHO Reporting System for Pancreatobiliary Cytopathology. Chapter 9.
- Pitman MB, Centeno BA, Reid MD, Siddiqui MT, Layfield LJ, Perez-Machado M, Weynand B, Stelow EB, Lozano MD, Fukushima N, Cree IA, Mehrotra R, Schmitt FC, Field AS. The World Health Organization Reporting System for Pancreaticobiliary Cytopathology. Acta Cytol. 2023;67(3):304-320. doi: 10.1159/000527912. Epub 2022 Dec 14. Erratum in: Acta Cytol. 2024;68(1):80. doi: 10.1159/000535800. PMID: 36516741.
- Kubota Y, Kawakami H, Natsuizaka M, Kawakubo K, Marukawa K, Kudo T, Abe Y, Kubo K, Kuwatani M, Hatanaka Y, Mitsuhashi T, Matsuno Y, Sakamoto N. CTNNB1 mutational analysis of solid-pseudopapillary neoplasms of the pancreas using endoscopic ultrasound-guided fine-needle aspiration and next-generation deep sequencing. J Gastroenterol. 2015 Feb;50(2):203-10. doi: 10.1007/s00535-014-0954-y. Epub 2014 Apr 4. PMID: 24700283.
- Rodriguez-Matta E, Hemmerich A, Starr J, Mody K, Severson EA, Colon-Otero G. Molecular genetic changes in solid pseudopapillary neoplasms (SPN) of the pancreas. Acta Oncol. 2020 Sep;59(9):1024-1027. doi: 10.1080/0284186X.2020.1792549. Epub 2020 Jul 16. PMID: 32672484; PMCID: PMC8081262.
- La Rosa S, Bongiovanni M. Pancreatic Solid Pseudopapillary Neoplasm: Key Pathologic and Genetic Features. Arch Pathol Lab Med. 2020 Jul 1;144(7):829-837. doi: 10.5858/arpa.2019-0473-RA. PMID: 31958381.
- Meriden Z, Shi C, Edil BH, Ellison T, Wolfgang CL, Cornish TC, Schulick RD, Hruban RH. Hyaline globules in neuroendocrine and solid-pseudopapillary neoplasms of the pancreas: a clue to the diagnosis. Am J Surg Pathol. 2011 Jul;35(7):981-8. doi: 10.1097/PAS.0b013e31821a9a14. PMID: 21677537; PMCID: PMC3283163.
- Mehta N, Modi L, Patel T, Shah M. Study of cytomorphology of solid pseudopapillary tumor of pancreas and its differential diagnosis. J Cytol. 2010 Oct;27(4):118-22. doi: 10.4103/0970-9371.73293. PMID: 21157561; PMCID: PMC3001197.
- Kim MJ, Jang SJ, Yu E. Loss of E-cadherin and cytoplasmic-nuclear expression of beta-catenin are the most useful immunoprofiles in the diagnosis of solid-pseudopapillary neoplasm of the pancreas. Hum Pathol. 2008 Feb;39(2):251-8. doi: 10.1016/j.humpath.2007.06.014. Epub 2007 Oct 24. PMID: 17959228.
- Guo Y, Yuan F, Deng H, Wang HF, Jin XL, Xiao JC. Paranuclear dot-like immunostaining for CD99: a unique staining pattern for diagnosing solid-pseudopapillary neoplasm of the pancreas. Am J Surg Pathol. 2011 Jun;35(6):799-806. doi: 10.1097/PAS.0b013e318219c036. PMID: 21566515.
- Pitman MB, Centeno BA, Ali SZ, Genevay M, Stelow E, Mino-Kenudson M, Castillo CF, Schmidt CM, Brugge WR, Layfield LJ. Standardized terminology and nomenclature for pancreatobiliary cytology: The Papanicolaou Society of Cytopathology Guidelines. Cytojournal. 2014 Jun 2;11(Suppl 1):3. doi: 10.4103/1742-6413.133343. PMID: 25191517; PMCID: PMC4153338.
- Wang J, Gerrard G, Poskitt B, Dawson K, Trivedi P, Foroni L, El-Bahrawy M. Targeted next generation sequencing of pancreatic solid pseudopapillary neoplasms show mutations in Wnt signaling pathway genes. Pathol Int. 2019 Apr;69(4):193-201. doi: 10.1111/pin.12778. Epub 2019 Feb 27. PMID: 30811747.
- Dinarvand P, Lai J. Solid Pseudopapillary Neoplasm of the Pancreas: A Rare Entity With Unique Features. Arch Pathol Lab Med. 2017 Jul;141(7):990-995. doi: 10.5858/arpa.2016-0322-RS. PMID: 28661210.