Case of the Month ...

A 77-year-old male presented with a prolonged history of bone pain, muscle weakness, and multiple fragility fractures. Laboratory studies revealed hypophosphatemia with renal phosphate wasting and elevated serum fibroblast growth factor 23 (FGF23), consistent with tumor-induced osteomalacia. Functional imaging with ⁶⁸Ga-DOTATATE PET/CT demonstrated DOTATATE-avid lesions in the cervical vertebral bodies at C5 and C6. A biopsy was performed, and touch preparation cytology smears were obtained for evaluation, with additional material submitted for histologic and ancillary studies.
Authors
- Yousif Abdelmoneim, MBBS1; Mitra Abdollahi Nesiani, MD1
- Aziza Nassar, MD, MPH2
- Andrew L. Folpe, MD2
Affiliations
1Department of Laboratory Medicine and Pathology, Mayo Clinic, Jacksonville, Florida, USA
2Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota, USA
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
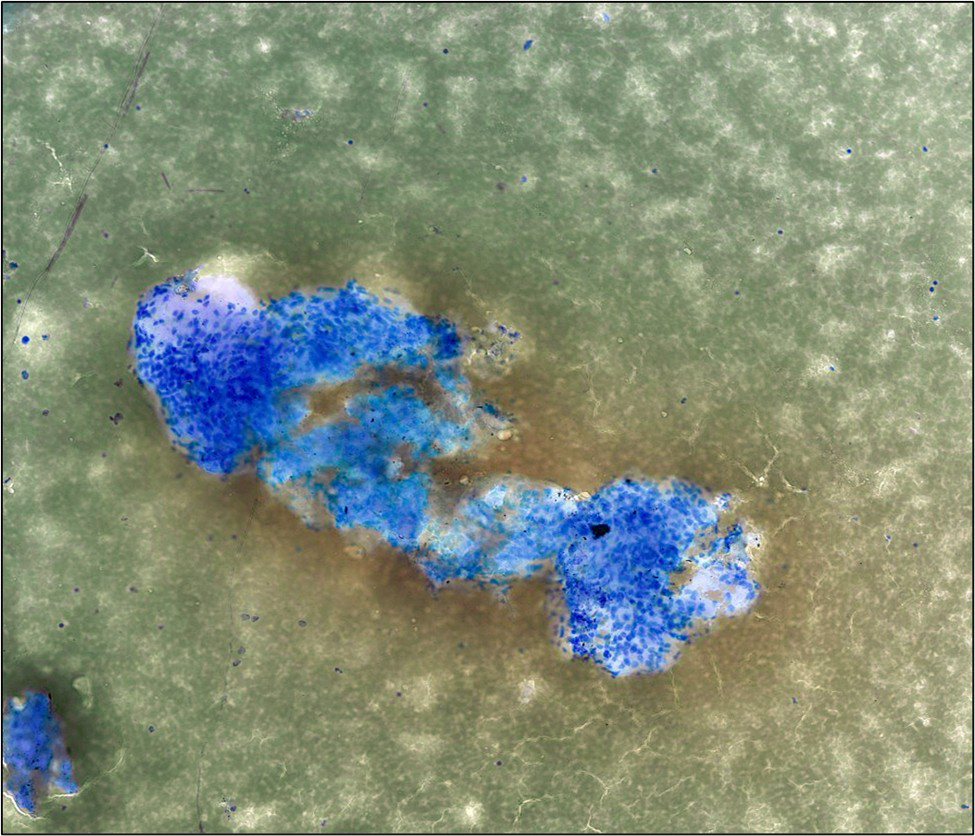
- Figure 1: Bone, cervical spine (C5–C6) lesion, touch preparation smear, Diff-Quik stain, 100×magnification.
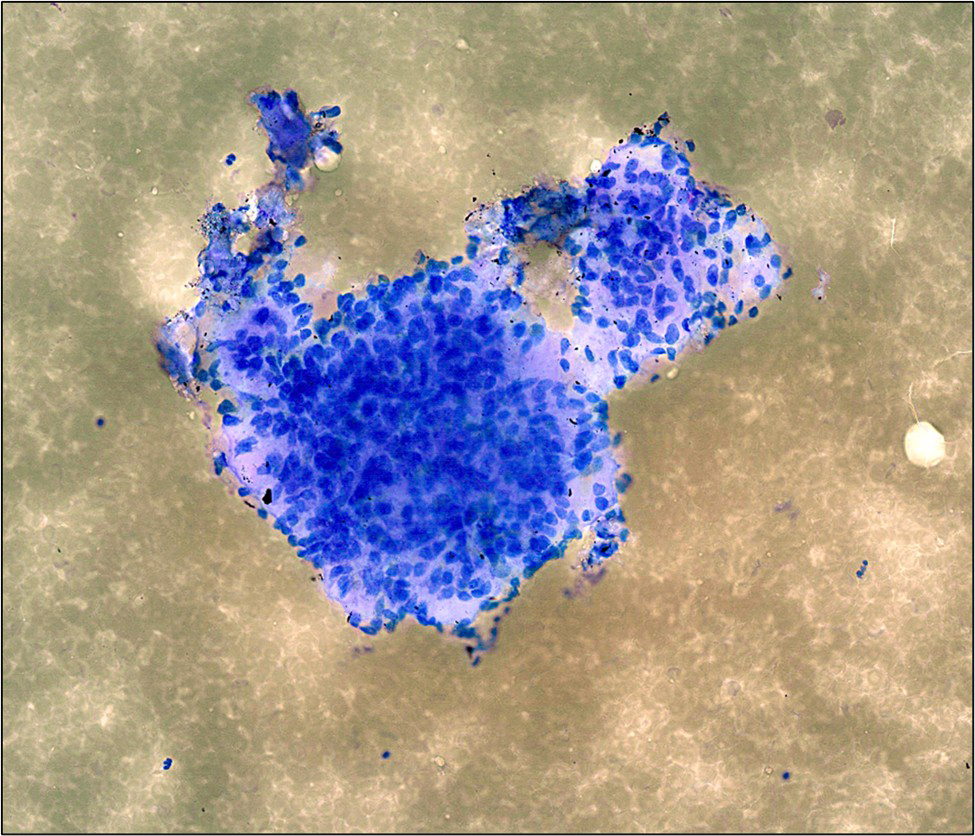
- Figure 2: Bone, cervical spine (C5–C6) lesion, touch preparation smear, Diff-Quik stain, 200×magnification.
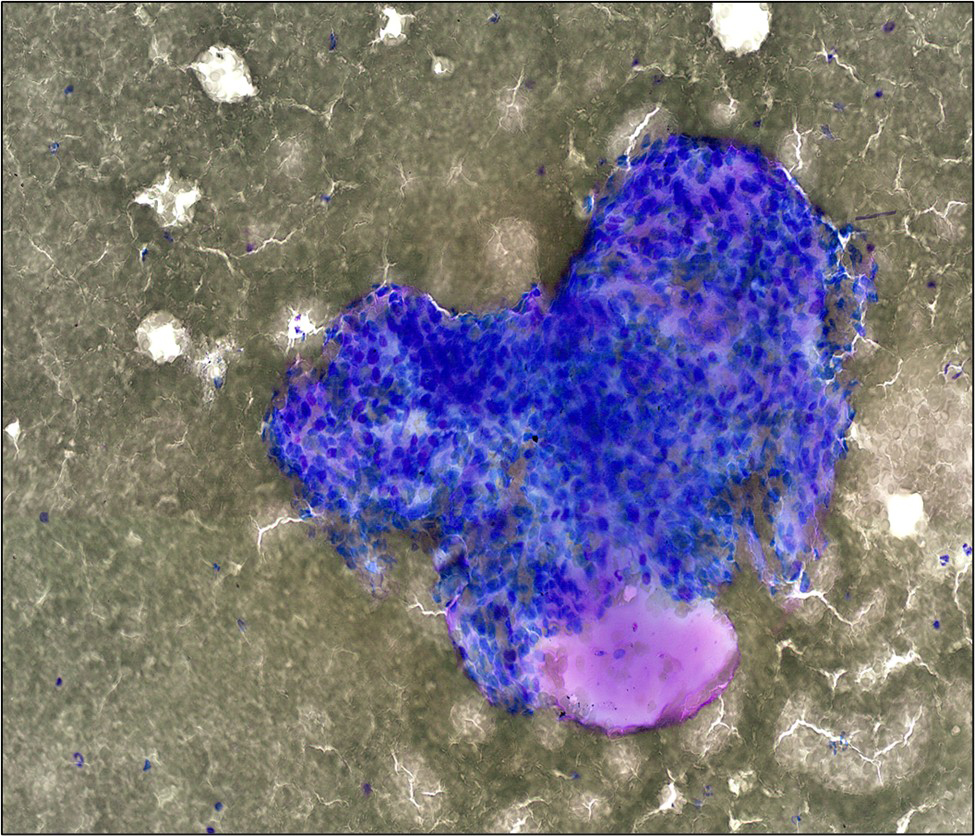
- Figure 3: Bone, cervical spine (C5–C6) lesion, touch preparation smear, Diff-Quik stain, 200×magnification.
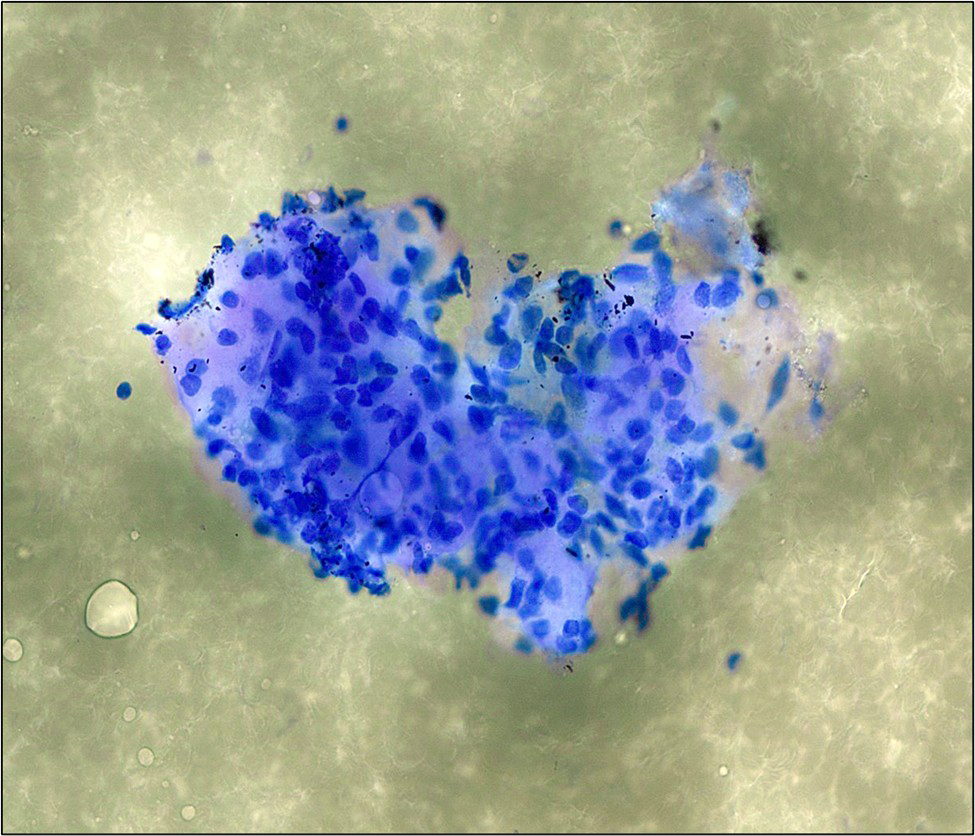
- Figure 4: Bone, cervical spine (C5–C6) lesion, touch preparation smear, Diff-Quik stain, 400×magnification.
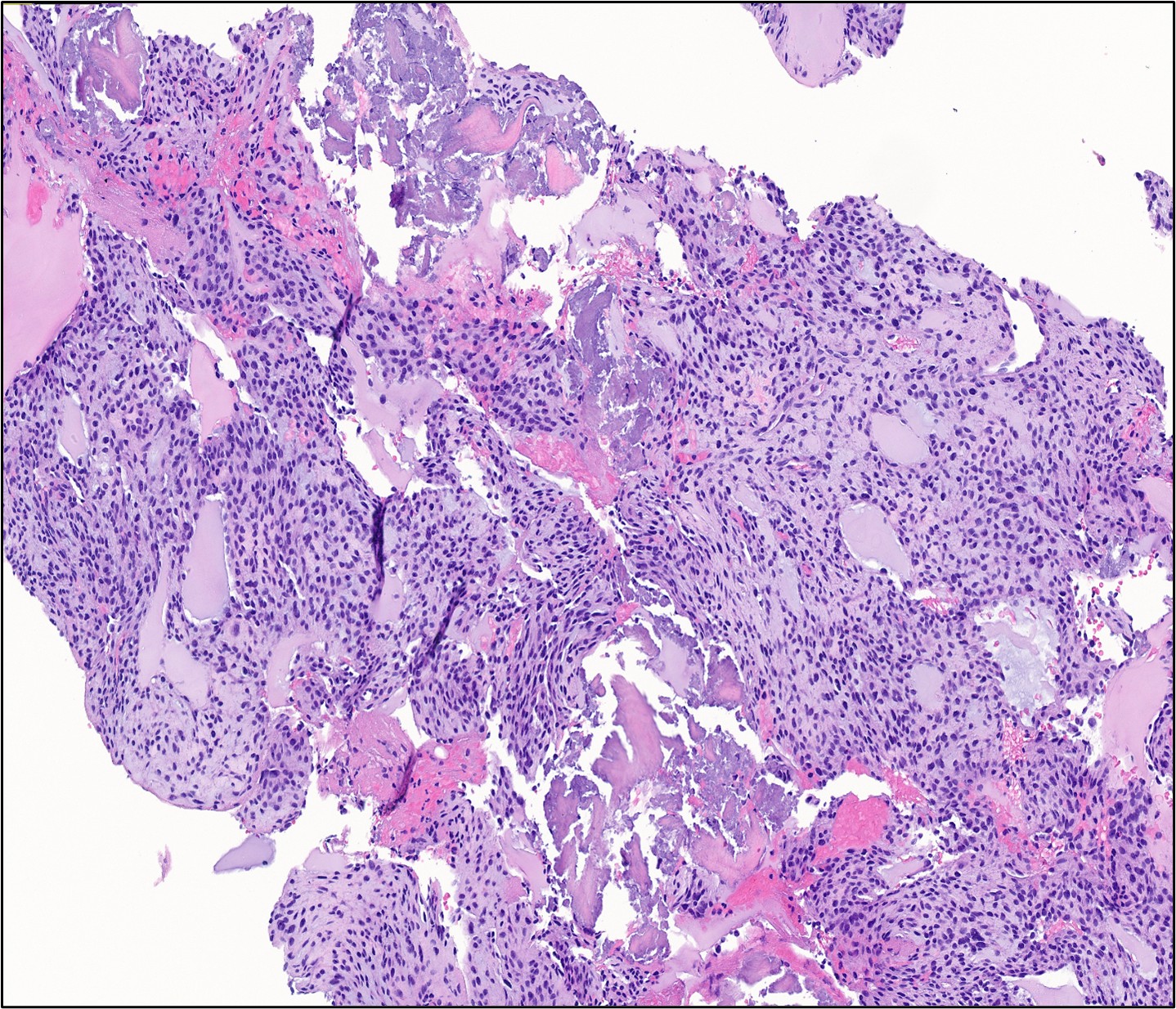
- Figure 5: Bone, cervical spine (C5–C6) lesion, biopsy, hematoxylin and eosin (H&E) stain, 200× magnification
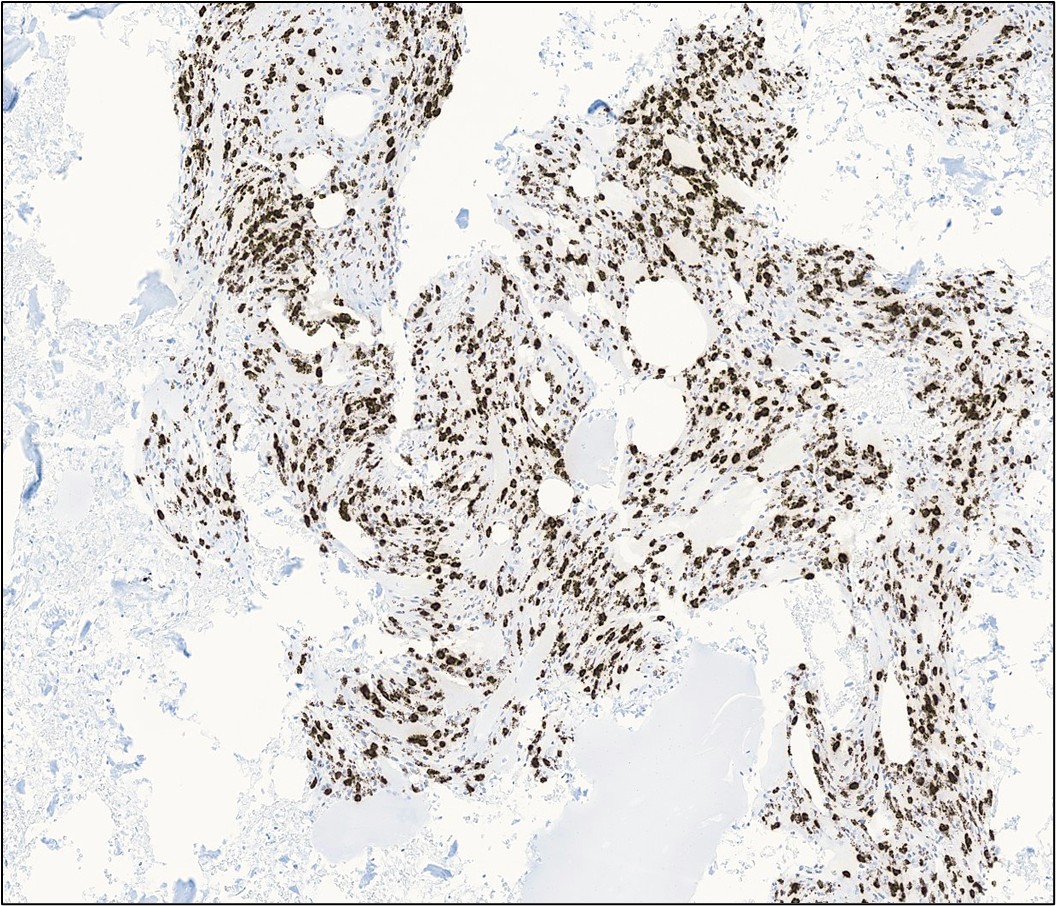
- Figure 6: Bone, cervical spine (C5–C6) lesion, biopsy, FGF23 mRNA chromogenic in situ hybridization (CISH), 100× magnification.
Questions:
- What is the most appropriate adequacy interpretation for this touch prep specimen?
- Non-diagnostic
- Atypical cells present
- Positive for neoplasm
- Positive for sarcoma
- Positive for benign spindle cell lesion
- Which of the following cytomorphologic features is most characteristic of phosphaturic mesenchymal tumor on touch prep?
- Highly pleomorphic cells with frequent mitoses
- Bland spindle cells with fibrillary stromal matrix and osteoclast-type giant cells
- Small round blue cells with nuclear molding
- Epithelioid cells with abundant eosinophilic cytoplasm
- Signet ring cells with cytoplasmic mucin vacuoles
- In the context of tumor-induced osteomalacia with hypophosphatemia and elevated FGF23, which ancillary test is most specific for confirming the diagnosis?
- Immunohistochemistry for S100 and SOX10
- FGF23 mRNA chromogenic in situ hybridization (CISH)
- STAT6 immunohistochemistry
- MDM2 FISH amplification
- Cytokeratin AE1/AE3 immunohistochemistry
- FGFR2 FISH was negative in this case. What is the significance of this finding?
- It excludes the diagnosis of phosphaturic mesenchymal tumor
- It confirms the tumor is benign
- It does not exclude the diagnosis, as FGFR rearrangements are present in only a subset of cases
- It indicates the tumor will not respond to surgical resection
- It suggests an alternative diagnosis such as solitary fibrous tumor
- Which of the following is the most important differential diagnosis to exclude in a bland spindle cell neoplasm presenting with DOTATATE avidity?
- Synovial sarcoma
- Solitary fibrous tumor
- Peripheral nerve sheath tumor
- Chondrosarcoma
- Osteosarcoma
Answers:
Question 1
Correct answer is C. Positive for neoplasm.
Touch prep smears show a population of bland spindle cells with elongated nuclei, fine chromatin, and inconspicuous nucleoli. The cells have delicate cytoplasm and are arranged in short fascicles or loosely cohesive clusters within a fibrillary stromal matrix. The background is hemorrhagic. Importantly, there is no significant cytologic atypia, mitotic activity, or necrosis.
At the time of adequacy assessment, the bland cytologic features preclude a definitive diagnosis of sarcoma. The histologically benign appearance with absence of significant atypia or mitotic activity also makes "positive for benign spindle cell lesion" inappropriate, as the clinical and radiologic context strongly suggests a neoplastic process requiring further characterization. "Positive for neoplasm" represents the most accurate adequacy interpretation, consistent with the final pathologic diagnosis, allowing for appropriate ancillary studies to achieve definitive classification.
Question 2
Correct answer is B. Bland spindle cells with fibrillary stromal matrix and osteoclast-type giant cells.
Phosphaturic mesenchymal tumor (PMT) is a rare neoplasm that causes tumor-induced osteomalacia (TIO) through secretion of FGF23. The cytologic literature on this entity is extremely limited, with only a handful of cases reported. The cytomorphologic features of phosphaturic mesenchymal tumor on touch preparation are relatively nonspecific but include bland spindle cells with elongated nuclei, fine chromatin, inconspicuous nucleoli, and delicate cytoplasm. These cells are arranged singly or in loose clusters within a fibrillary, stromal-rich (osteoid-like) matrix. Osteoclast-type giant cells are frequently present and represent an important diagnostic clue. The background typically shows hemorrhage. Importantly, there is no significant cytologic atypia, mitotic activity, or necrosis. Ultimately, this amalgam of cytologic findings can mimic numerous benign and malignant spindle cell neoplasms including solitary fibrous tumor, peripheral nerve sheath tumor, low-grade fibrosarcoma, and chondromyxoid fibroma. The key to diagnosis is clinical correlation with the biochemical findings of hypophosphatemia, elevated FGF23, and osteomalacia, combined with radiologic features showing DOTATATE avidity on functional imaging. The histologic hallmarks of PMT include bland spindled cells, a conspicuous vascular network, and the pathognomonic "smudgy" or "grungy" basophilic calcified matrix.
Recognition of phosphaturic mesenchymal tumor on cytology and touch prep specimens is critical, as complete surgical resection cures the intractable osteomalacia. Following successful resection, serum phosphorus typically normalizes within days. Cytopathologists should maintain a high index of suspicion for this entity when evaluating bland spindle cell lesions in patients with bone pain, fractures, and metabolic abnormalities suggestive of tumor-induced osteomalacia.
This patient was treated with phosphorus supplementation and activated vitamin D (calcitriol) for four months prior to surgery, resulting in significant clinical improvement with enhanced bone healing. Definitive treatment consisted of C5-C6 corpectomy with cage placement, C4-C7 anterior plating, and percutaneous posterior instrumented fusion. Complete surgical resection is curative in over 90% of cases.
Answer A (highly pleomorphic cells with frequent mitoses) would suggest a high-grade sarcoma. Answer C (small round blue cells with nuclear molding) would suggest small cell carcinoma or other small round blue cell tumors. Answer D (epithelioid cells with abundant eosinophilic cytoplasm) would suggest an epithelioid neoplasm such as epithelioid sarcoma or melanoma. Answer E (signet ring cells with cytoplasmic mucin vacuoles) would suggest adenocarcinoma.
Question 3
Correct answer is B. FGF23 mRNA chromogenic in situ hybridization (CISH).
FGF23 mRNA CISH is the most specific ancillary test for confirming the diagnosis of phosphaturic mesenchymal tumor. While FGF23 immunohistochemistry has historically been used, it suffers from variable sensitivity and specificity due to the secretory nature of FGF23 protein. FGF23 mRNA CISH directly detects transcription of the FGF23 gene within tumor cells and has demonstrated superior sensitivity and specificity compared to immunohistochemistry. In this case, FGF23 mRNA CISH was positive, confirming that the tumor cells are actively producing FGF23, the causative factor in tumor-induced osteomalacia.
Answer A (S100, SOX10) would be appropriate for peripheral nerve sheath tumors. Answer C (STAT6) would identify solitary fibrous tumor. Answer D (MDM2 FISH) would be used for well-differentiated/dedifferentiated liposarcoma. Answer E (cytokeratin) would be appropriate for epithelial neoplasms.
Question 4
Correct answer is C. It does not exclude the diagnosis, as FGFR rearrangements are present in only a subset of cases.
FGFR gene rearrangements, most commonly FN1-FGFR1 fusions, are identified in approximately 40-60% of phosphaturic mesenchymal tumors. Other FGFR rearrangements including FN1-FGFR2 have also been reported but are less common. A significant proportion of PMTs lack any detectable FGFR rearrangement. Therefore, a negative FGFR2 FISH result does not exclude the diagnosis. In this case, the diagnosis is firmly established by the combination of clinical findings (hypophosphatemia, elevated FGF23, osteomalacia), radiologic features (DOTATATE avidity), histologic features (bland spindle cells with characteristic matrix), and positive FGF23 mRNA CISH. While the negative FGFR2 result does not exclude the diagnosis, it does have therapeutic implications: in the event of unresectable or recurrent disease, FGFR inhibitor therapy would not be a molecularly targeted option for this patient. Alternative therapies for refractory disease include peptide receptor radionuclide therapy (¹⁷⁷Lu-DOTATATE) given the DOTATATE avidity of the tumor.
Answer A is incorrect because a negative FGFR result does not exclude PMT. Answer B is incorrect because FGFR status does not determine benign versus malignant behavior. Answer D is incorrect because surgical resection remains the definitive curative treatment regardless of FGFR status. Answer E is incorrect because a negative FGFR result does not suggest an alternative diagnosis when the clinical, histologic, and FGF23 CISH findings are concordant. However, the absence of an FGFR rearrangement does mean that FGFR inhibitor therapy would not be a targeted option in the event of unresectable or recurrent disease.
Question 5
Correct answer is B. Solitary fibrous tumor.
Solitary fibrous tumor (SFT) is the most important differential diagnosis to exclude in a bland spindle cell neoplasm presenting with DOTATATE avidity. Both PMT and SFT can present as bland spindle cell tumors with prominent vasculature and can demonstrate DOTATATE uptake on PET/CT imaging. Histologically, both tumors show bland spindle cells arranged in a patternless architecture with a prominent vascular network. The key distinguishing features are: (1) clinical context—PMT presents with tumor-induced osteomalacia (hypophosphatemia, elevated FGF23), while SFT does not cause metabolic abnormalities; (2) histologic features—PMT characteristically shows "smudgy" or "grungy" basophilic calcified matrix, which is absent in SFT; (3) immunohistochemistry—SFT is positive for STAT6 (nuclear) and CD34, while PMT is negative for these markers; and (4) molecular studies—FGF23 mRNA CISH is positive in PMT and negative in SFT.
Answer A (synovial sarcoma) typically shows more cellular atypia and would be positive for TLE1 and may show SS18 rearrangement. Answer C (peripheral nerve sheath tumor) would be positive for S100 and SOX10. Answer D (chondrosarcoma) would show chondroid matrix and different cytomorphology. Answer E (osteosarcoma) would show malignant osteoid production and significant cytologic atypia.
References
- Folpe AL. Phosphaturic mesenchymal tumors: a review and update. InSeminars in diagnostic pathology 2019 Jul 1 (Vol. 36, No. 4, pp. 260-268). WB Saunders.
- Monappa V, Naik AM, Mathew M, Rao L, Rao SK, Ramachandra L, PadmaPriya J. Phosphaturic mesenchymal tumour of the mandible–the useful criteria for a diagnosis on fine needle aspiration cytology. Cytopathology. 2014 Feb;25(1):54-6.
- Folpe AL, Fanburg-Smith JC, Billings SD, Bisceglia M, Bertoni F, Cho JY, Econs MJ, Inwards CY, De Beur SM, Mentzel T, Montgomery E. Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. The American journal of surgical pathology. 2004 Jan 1;28(1):1-30.
- Lee JC, Su SY, Changou CA, Yang RS, Tsai KS, Collins MT, Orwoll ES, Lin CY, Chen SH, Shih SR, Lee CH. Characterization of FN1–FGFR1 and novel FN1–FGF1 fusion genes in a large series of phosphaturic mesenchymal tumors. Modern Pathology. 2016 Nov 1;29(11):1335-46.
- Bahrami A, Weiss SW, Montgomery E, Horvai AE, Jin L, Inwards CY, Folpe AL. RT-PCR analysis for FGF23 using paraffin sections in the diagnosis of phosphaturic mesenchymal tumors with and without known tumor induced osteomalacia. The American journal of surgical pathology. 2009 Sep 1;33(9):1348-54.
- Carter JM, Caron BL, Dogan A, Folpe AL. A novel chromogenic in situ hybridization assay for FGF23 mRNA in phosphaturic mesenchymal tumors. The American journal of surgical pathology. 2015 Jan 1;39(1):75-83.
- Lee JC, Jeng YM, Su SY, Wu CT, Tsai KS, Lee CH, Lin CY, Carter JM, Huang JW, Chen SH, Shih SR. Identification of a novel FN1–FGFR1 genetic fusion as a frequent event in phosphaturic mesenchymal tumour. The Journal of pathology. 2015 Mar;235(4):539-45.