Case of the Month ...

A 25-year-old male presented with a slowly enlarging, painless mass on the right cheek. Imaging demonstrated a superficial well-circumscribed mass anterior to but not directly connected to the parotid gland. Fine-needle aspiration (FNA) was performed for diagnostic evaluation. Cytospin slides (Papanicolaou stain) and a cell block (H&E stain) were prepared.
Cytospin and cell block section are shown below, along with representative immunohistochemical stains.
Authors
- Arkar Htoo, MD, FCAP. Cytopathology Fellow. Robert J. Tomsich Department of Pathology & Laboratory Medicine, Diagnostic Institute, Cleveland Clinic Foundation.
- Juan Xing, MD, PhD. Associate Professor. Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
- Figure 1: FNA of right cheek mass, cytospin, Pap stained, 40× magnification.
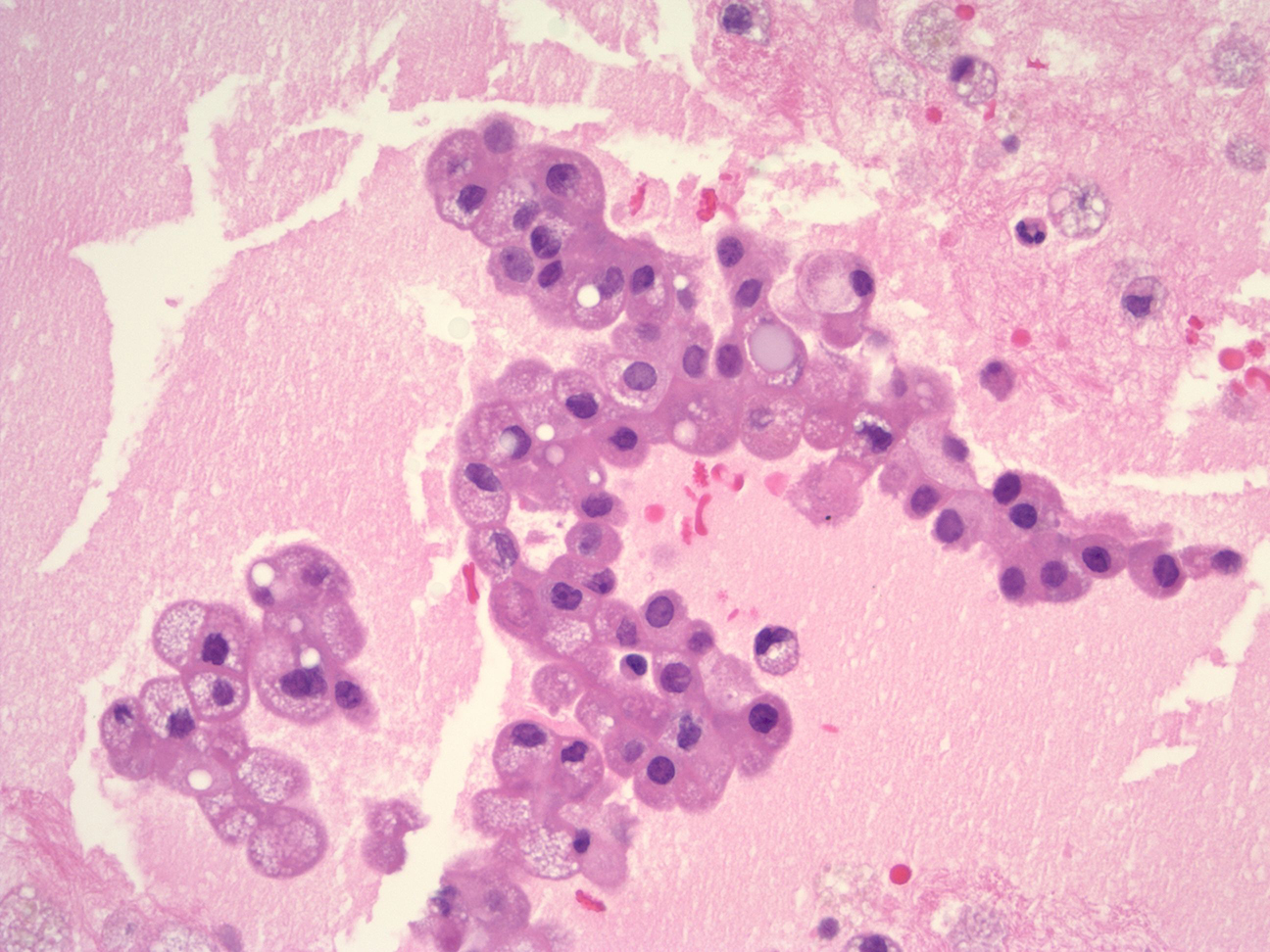
- Figure 2: Cell block, H&E stain, 40× magnification.
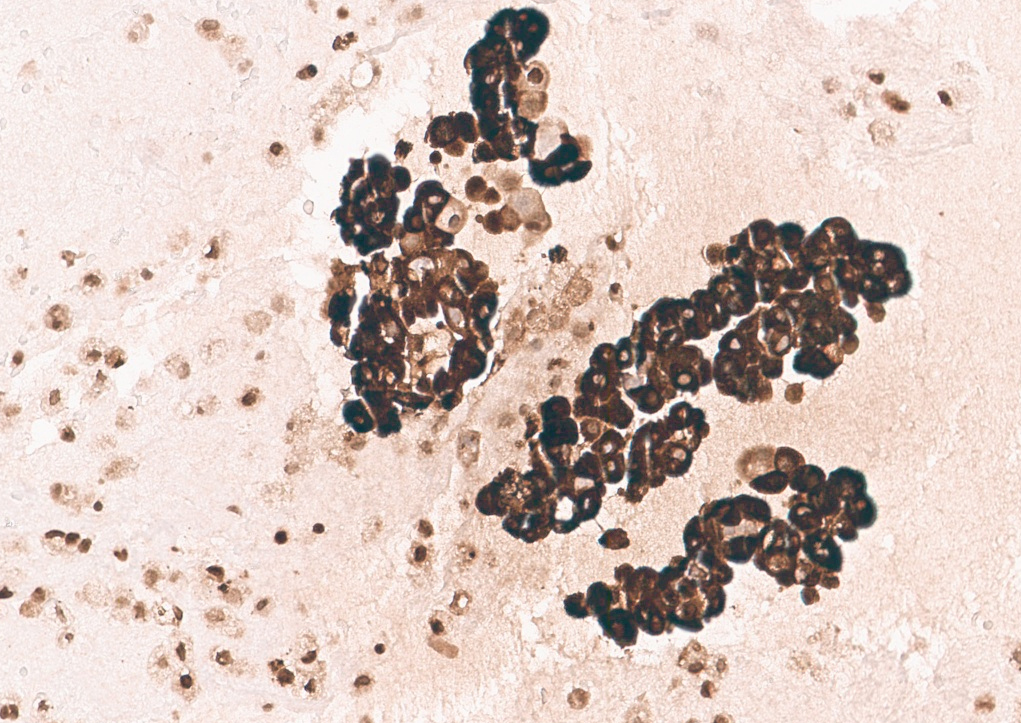
- Figure 3: Cell block, GATA3 immunohistochemical stain, 20× magnification.
- Figure 4: Cell block, Mammaglobin immunohistochemical stain, 20× magnification.
- Figure 5: Cell block, S100 immunohistochemical stain, 20× magnification.
- Figure 6: Cell block, Pan-TRK immunohistochemical stain, 20× magnification.
Questions:
- Based on the cytomorphology, immunohistochemistry, and clinical information, what is the correct diagnosis for this patient?
- Secretory carcinoma
- Oncocytic neoplasm
- Mucoepidermoid carcinoma
- Acinic cell carcinoma
- Salivary duct carcinoma
- Which cytomorphologic feature is most characteristic of secretory carcinoma on FNA?
- Prominent keratinization and dense cytoplasm
- Abundant granular basophilic cytoplasm with zymogen granules
- Papillary clusters with vacuolated cytoplasm and background macrophages
- Biphasic ductal and myoepithelial cell population
- Marked nuclear pleomorphism with comedo necrosis
- Which immunohistochemical profile best supports the diagnosis of secretory carcinoma?
- DOG1 positive, S100 negative
- Mammaglobin positive, S100 positive, GATA3 positive
- Androgen receptor positive, HER2 positive
- p63 diffuse positive
- SOX10 negative, mammaglobin negative
- Secretory carcinoma of the salivary gland is most commonly associated with which molecular alteration?
- CRTC1-MAML2 fusion
- MYB-NFIB fusion
- ETV6-NTRK3 fusion
- HRAS mutation
- SMARCB1 loss
Answers:
Question 1: Correct answer: A. Secretory carcinoma.
Secretory carcinoma of the salivary gland, previously known as “mammary analogue secretory carcinoma,” is a distinct low-grade malignant epithelial neoplasm recognized in the WHO Classification of Head and Neck Tumors.1 On fine-needle aspiration, it typically demonstrates bland-appearing cuboidal or polygonal cells arranged in papillary, microcystic, or tubular structures. The neoplastic cells demonstrate eccentrically located round to oval nuclei, smooth nuclear contours, and conspicuous nucleoli. The cytoplasm is characteristically abundant, eosinophilic to vacuolated (foamy), with intracytoplasmic vacuoles that may be large and easily appreciable. A background rich in macrophages and proteinaceous secretions is common and reflects secretory material.2
Question 2: Correct answer: C. Papillary clusters with vacuolated cytoplasm and background macrophages.
The main differential diagnoses for salivary gland secretory carcinoma include acinic cell carcinoma, low-grade mucoepidermoid carcinoma, oncocytic neoplasms, and low-grade salivary duct carcinoma. Acinic cell carcinoma contains distinct intracytoplasmic zymogen granules. Oncocytic tumors exhibit centrally located round nuclei with prominent nucleoli and abundant finely granular eosinophilic cytoplasm. In contrast to the mucinous cells seen in mucoepidermoid carcinoma, the vacuolated cells in secretory carcinoma are multivacuolated and lack a squamous cell component. Additionally, secretory carcinoma is often characterized by papillary structures and more prominent cytoplasmic vacuoles. The combination of papillary architecture, vacuolated cytoplasm, and macrophage-rich background is most characteristic of secretory carcinoma in cytology specimens.
Option A describes squamous differentiation.
Option B is more typical of acinic cell carcinoma, which shows granular basophilic cytoplasm due to zymogen granules.
Option D suggests pleomorphic adenoma or another biphasic neoplasm.
Option E describes high-grade salivary duct carcinoma.
Question 3: Correct answer: B. Mammaglobin positive, S100 positive, GATA3 positive.
Secretory carcinoma demonstrates a characteristic immunophenotype with diffuse co-expression of S100 protein and mammaglobin, along with GATA3 positivity. SOX10 may be positive, often focally.2 DOG1 is typically negative, helping to distinguish this entity from acinic cell carcinoma. Lack of androgen receptor (AR) expression helps exclude salivary duct carcinoma. p63 negativity supports the absence of a basal/myoepithelial phenotype. Pan-TRK immunohistochemistry is frequently positive and serves as a surrogate marker for underlying NTRK gene fusion. Thus, the combined S100, mammaglobin, GATA3, and Pan-TRK positivity best supports a diagnosis of secretory carcinoma.
Option A (DOG1 positive) favors acinic cell carcinoma.
Option C (AR and HER2 positive) supports salivary duct carcinoma.
Option D (diffuse p63 positivity) indicates basal/myoepithelial differentiation.
Option E is consistent with SMARCB1-deficient tumors.Question 4: Correct answer: C. ETV6-NTRK3 fusion.
Secretory carcinoma is defined by ETV6 gene rearrangement, most commonly the ETV6-NTRK3 fusion.3 This molecular alteration results in constitutive activation of TRK signaling pathways and is considered pathognomonic. Pan-TRK positivity on immunohistochemistry reflects expression of the fusion protein and may be used as a screening tool, with confirmation by FISH, RT-PCR, or next-generation sequencing.
Identification of NTRK fusion has important therapeutic implications, as TRK inhibitors have demonstrated clinical efficacy in advanced or unresectable tumors.4 Recognition of this entity on cytology specimens is critical to ensure accurate classification, appropriate ancillary testing, and optimal patient management.
Option A (CRTC1-MAML2 fusion) is characteristic of mucoepidermoid carcinoma.
Option B (MYB-NFIB fusion) is typical of adenoid cystic carcinoma.
Option D (HRAS mutations) may be seen in epithelial-myoepithelial carcinoma.
Option E (SMARCB1 loss) is associated with certain myoepithelial carcinomas and other SWI/SNF-deficient neoplasms.References
- WHO Classification of Head and Neck Tumors. International Agency for Research on Cancer; 2022.
- Wiles AB, Gabrielson M, Baloch ZW, et al. Secretory carcinoma of the salivary gland, a rare entity: An international multi-institutional study. Cancer Cytopathol. 2022;130(9):684-694. doi:10.1002/cncy.22574
- Xu B, Viswanathan K, Umrau K, et al. Secretory carcinoma of the salivary gland: a multi-institutional clinicopathologic study of 90 cases with emphasis on grading and prognostic factors. Histopathology. 2022;81(5):670-679. doi:10.1111/his.14772
- Willis C, Au T, Hejazi A, et al. Clinical characteristics and treatment patterns of patients with NTRK fusion-positive solid tumors: A multisite cohort study at US academic cancer centers. J Manag Care Spec Pharm. 2024;30(7):672-683. doi:10.18553/jmcp.2024.30.7.672