Case of the Month ...

A 71-year-old female presented with a non-tender right forearm mass that has grown over the last 6 months. No history of trauma or injury to the area was noted. An MRI study revealed a 6.8 x 2.7 x 2.0 cm subcutaneous lobulated, multiseptated enhancing mass suspicious for leiomyosarcoma or liposarcoma. A percutaneous ultrasound-guided core needle biopsy was performed with cytology-assisted rapid onsite assessment via performed touch preparations.
Authors
- Sandra Rivera, DO and Y. Helen Zhang, MD. Department of Pathology and Laboratory Medicine. University of Texas Health Science Center at Houston, Houston, TX.
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
- Figure 1: Touch preparation, Diff-Quik stain, 400x
- Figure 2: Touch preparation, Papanicolaou stain, 200x
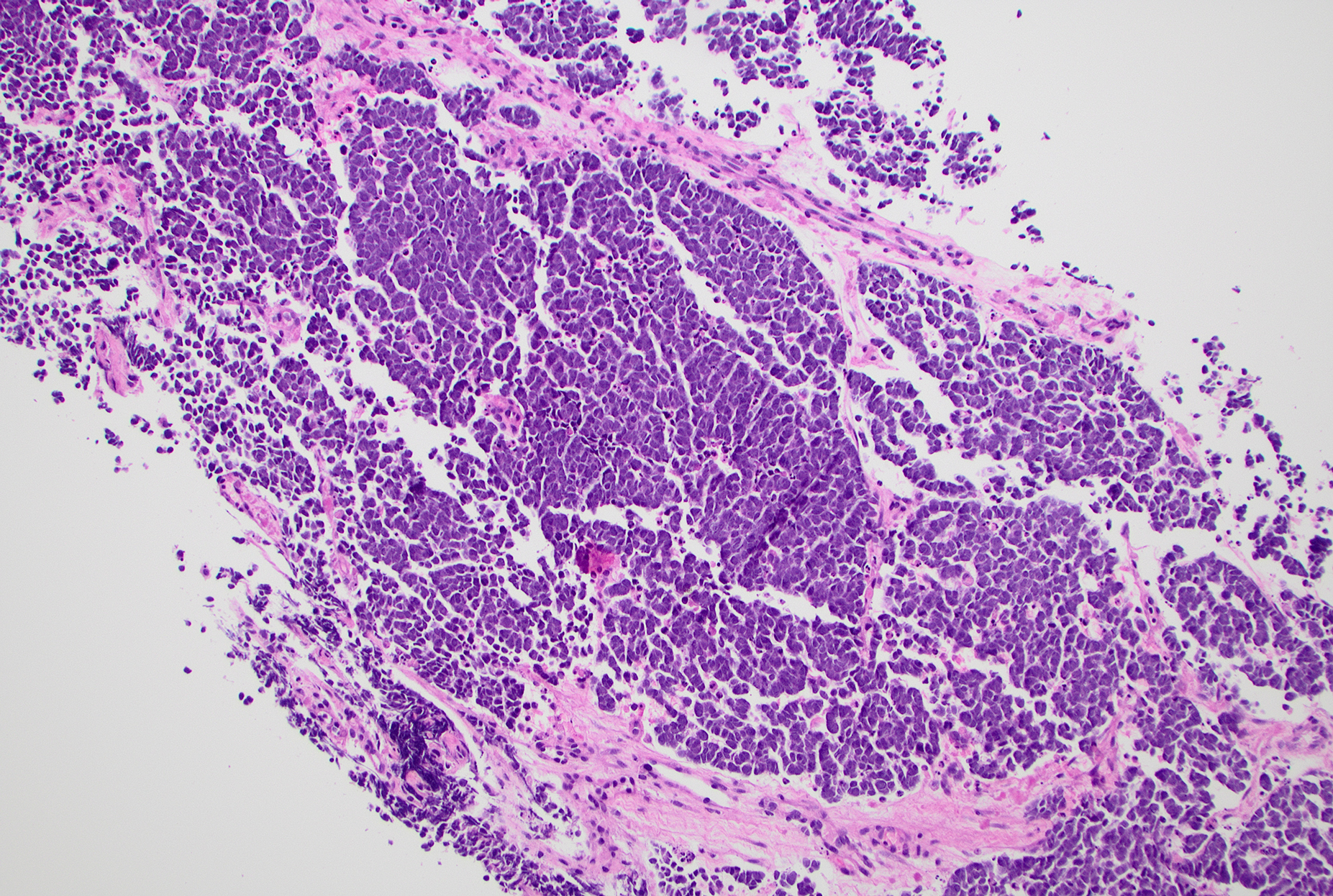
- Figure 3: Core biopsy of forearm mass, H&E stain, 100x
- Figure 4: Core biopsy, CK20 immunostain, 400x
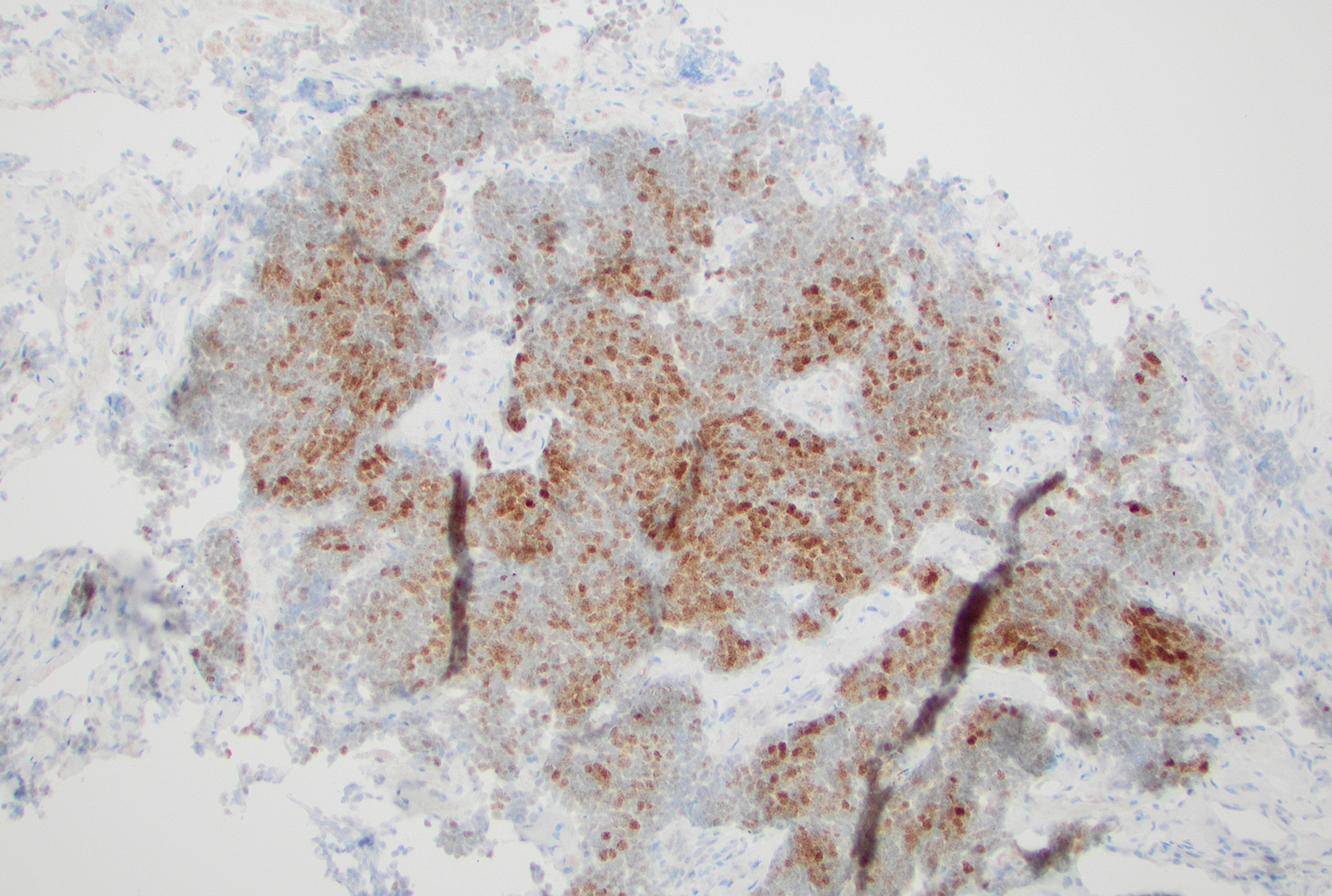
- Figure 5: Core biopsy, INSM1 immunostain, 100x
- Figure 6: Core biopsy, MCPyV immunostain, 100x
Questions:
- What is the most likely diagnosis based on the above clinical history, cytomorphology and immunoprofile?
- Atypical fibroxanthoma
- Basal cell carcinoma
- Ewing sarcoma
- Merkel cell carcinoma
- Lymphoma
- Which of the following morphologic and immunohistochemical features is NOT regarded as a key characteristic of this neoplasm?
- Mitotic figures and apoptotic bodies
- Discohesive tumor cells
- Tumor cell size may vary between small to medium and large
- Finely speckled chromatin pattern
- Paranuclear dot-like staining with CK20
- What is the immunohistochemical (IHC) stain that would likely be NEGATIVE in this lesion?
- TTF-1
- Chromogranin
- Synaptophysin
- CK20
- INSM1
- Why is the status of MCPyV (Merkel cell polyomavirus) important?
- Prognosis
- Treatment
- Staging
- Different genetic profiles
Answers:
Question 1: Correct Answer is D
The touch preparation and biopsy slides (Figures 1–3) show a small blue cell neoplasm composed of loosely cohesive and dispersed neoplastic cells with high nuclear-to-cytoplasmic ratios and fine, stippled chromatin. Nuclear molding is present. Immunohistochemical stains on the biopsy specimen reveal that these neoplastic cells are positive for CK20 (Figure 4, paranuclear dot-like pattern), CAM5.2, INSM1 (Figure 5), synaptophysin, chromogranin, and MCPyV (Figure 6), while negative for CD45, S100, TdT, CD34, desmin, p63, and CD99. The overall cytomorphological findings, along with the immunoprofile, are consistent with Merkel cell carcinoma (MCC). MCC is a fast-growing dermal tumor characterized by neuroendocrine cytology and an immunophenotype of neuroendocrine differentiation. The tumor predominantly affects elderly White individuals and those who are immunosuppressed.
Atypical fibroxanthoma (AFX) is a dermal-based skin tumor typically seen in elderly adults. It is characterized by pleomorphic, spindle, epithelioid, and multinucleated cells with numerous mitotic figures that mimic aggressive sarcomas; however, AFX is usually negative for cytokeratin.
In contrast, basal cell carcinoma demonstrates nests of small, basaloid cells with large nuclei, minimal cytoplasm, peripheral palisading, and tumor-stromal retraction artifacts. These tumors are negative for CK20, chromogranin, and synaptophysin.
When superficial, Ewing sarcoma can also be localized to the dermis with similar cytomorphology. While focal low-molecular-weight keratin is observed in one-third of Ewing sarcoma cases, these cells typically show diffuse, strong membranous staining for CD99 and are positive for FLI-1, ERG, and NKX2-2.
Finally, lymphoma cells are discohesive and typically express lymphoid markers, and are negative for CK20 and neuroendocrine markers.Question 2: Correct Anwer is B
MCC is a highly aggressive primary cutaneous neuroendocrine malignancy with an expansile, nodular, or infiltrative growth pattern. Architecturally, these tumors are characterized by sheets, nests, or occasional trabecular arrangements of monomorphic cells.
The cytologic features include a spectrum of small to intermediate and large cells. The neoplastic cells display high nuclear-to-cytoplasmic ratios and "salt-and-pepper" (fine stippled) chromatin with numerous mitotic figures and apoptotic bodies. Diagnostic confirmation relies on a specific immunohistochemical profile, most reliably indicated by a characteristic perinuclear dot-like staining for CK20 (positive in ~95% of cases) or neurofilament, alongside positivity for neuroendocrine markers such as INSM1, synaptophysin and chromogranin.Question 3: Correct Answer is A
Immunohistochemically, the tumor cells of MCC express epithelial markers (CAM5.2, AE1/AE3, CK20, BerEP4, EMA, occasionally CK7) and neuroendocrine markers (INSM1, chromogranin, synaptophysin, and CD56). They also express SATB2 and neurofilament. As previously mentioned, perinuclear dot-like staining for CK20 or neurofilament is the most reliable way to confirm MCC. TTF1 staining is almost always negative.Question 4: Correct Answer is A
Merkel cell polyomavirus (MCPyV) is found in approximately 80% of MCC tumors. Knowing the status of MCPyV is critical for managing Merkel cell carcinoma. Patients with MCPyV-positive tumors generally have significantly better overall and recurrence-free survival rates than those with virus-negative tumors. In MCPyV-negative MCCs, a high burden of TP53 and RB1 mutations and a UV radiation signature mutation profile have been found, in addition to a higher total mutation burden than virus-positive tumors.
Confirmation of the MCPyV status by immunohistochemistry and/or by molecular studies is essential for guiding personalized treatment plans and risk assessment.References:
- Messina J, Busam K, Scolyer RA, Tetzlaff M, Kervarrec T. Merkel Cell Carcinoma. World Health Organization (2026). Classification of Tumours: Skin tumours (5th ed.). https://tumourclassification.iarc.who.int/chaptercontent/64/39 (accessed January 14, 2026).
- Harms KL, Zhao L, Johnson B, Wang X, Carskadon S, Palanisamy N, Rhodes DR, Mannan R, Vo JN, Choi JE, Chan MP, Fullen DR, Patel RM, Siddiqui J, Ma VT, Hrycaj S, McLean SA, Hughes TM, Bichakjian CK, Tomlins SA, Harms PW. Virus-positive Merkel Cell Carcinoma Is an Independent Prognostic Group with Distinct Predictive Biomarkers. Clin Cancer Res. 2021 May 1;27(9):2494-2504. doi: 10.1158/1078-0432.CCR-20-0864. Epub 2021 Feb 5. PMID: 33547200; PMCID: PMC8995051.
- Walsh NM. Primary neuroendocrine (Merkel cell) carcinoma of the skin: morphologic diversity and implications thereof. Hum Pathol. 2001 Jul;32(7):680-9. doi: 10.1053/hupa.2001.25904. PMID: 11486166.
- Schadendorf D, Lebbé C, Zur Hausen A, Avril MF, Hariharan S, Bharmal M, Becker JC. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. Eur J Cancer. 2017 Jan;71:53-69. doi: 10.1016/j.ejca.2016.10.022. Epub 2016 Dec 14. PMID: 27984768.