Case of the Month ...
A 25-year-old male presented with a painful right axillary mass for one week, accompanied by fevers and night sweats. He denied skin injury, recent travel, or sick contacts. MRI revealed multiple lymph nodes in the area, with the largest node measuring up to 2.4 cm. Serology testing was negative for Rapid Plasma Reagin (RPR), HIV, and other acute conditions. The overall clinical impression was suspicious for lymphoma. An excisional biopsy with touch preparation of the largest lymph node was performed.
Authors
- Daphne Huynh, MD and Y. Helen Zhang, MD. Department of Pathology and Laboratory Medicine. University of Texas Health Science Center at Houston, Houston, TX.
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6
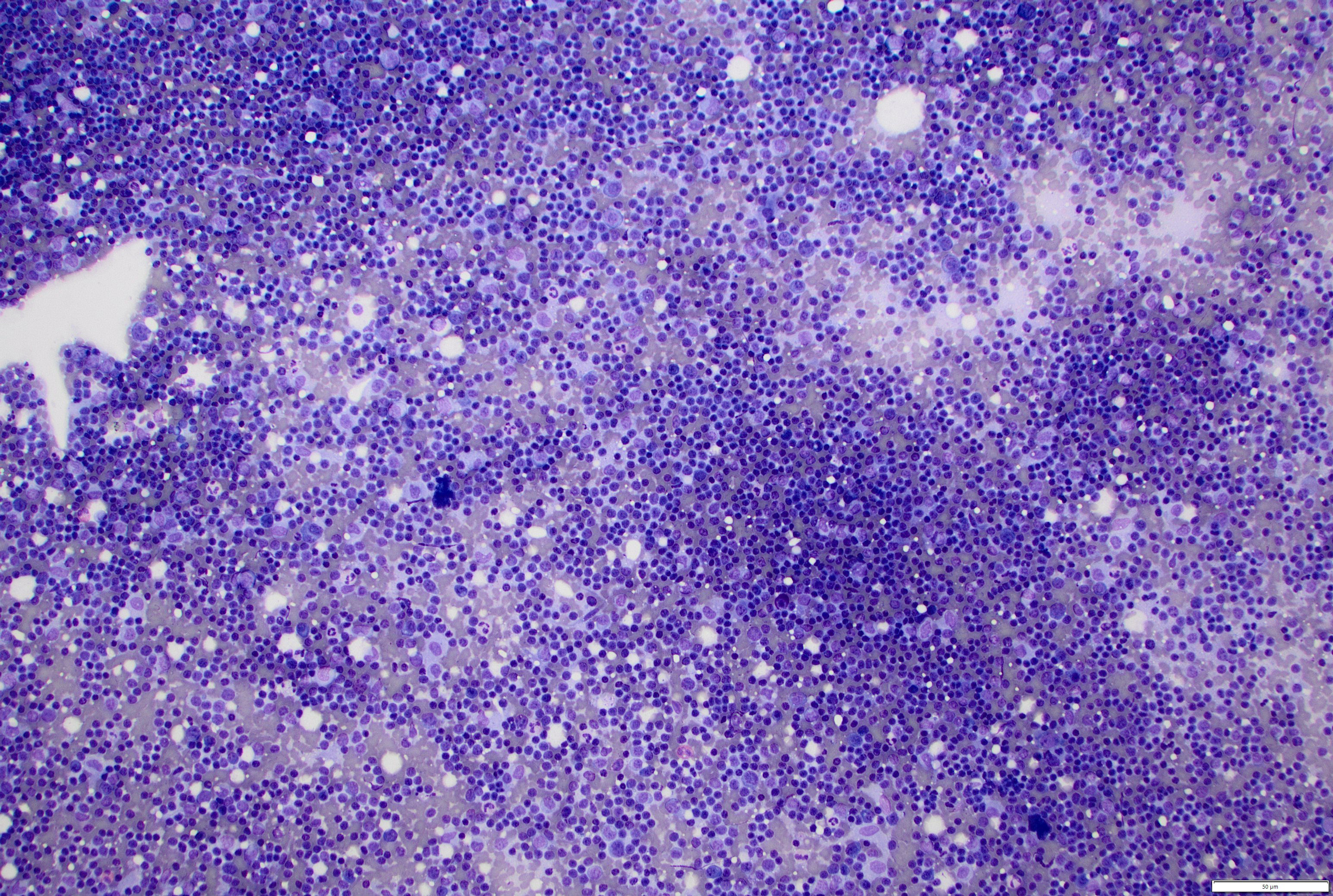
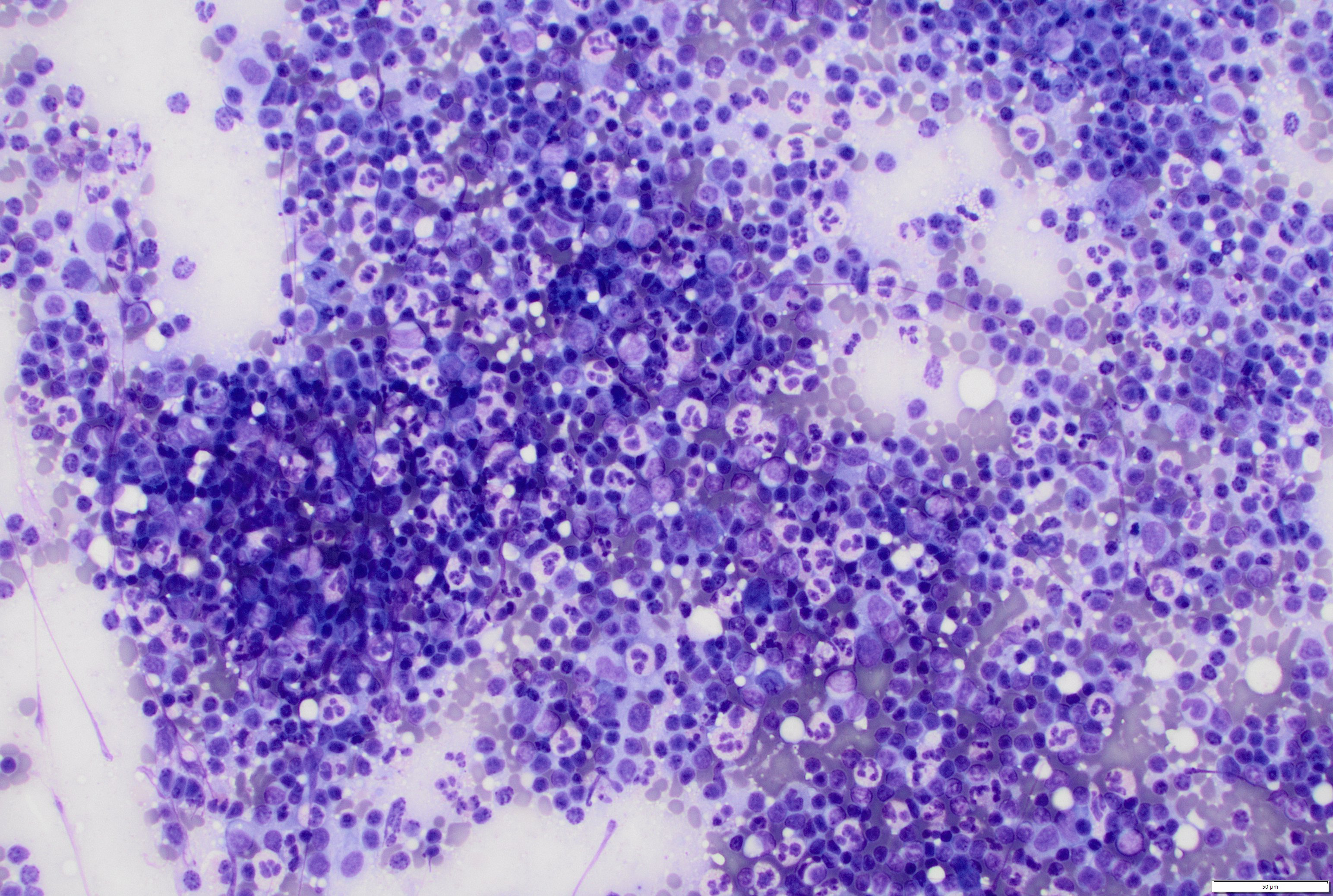
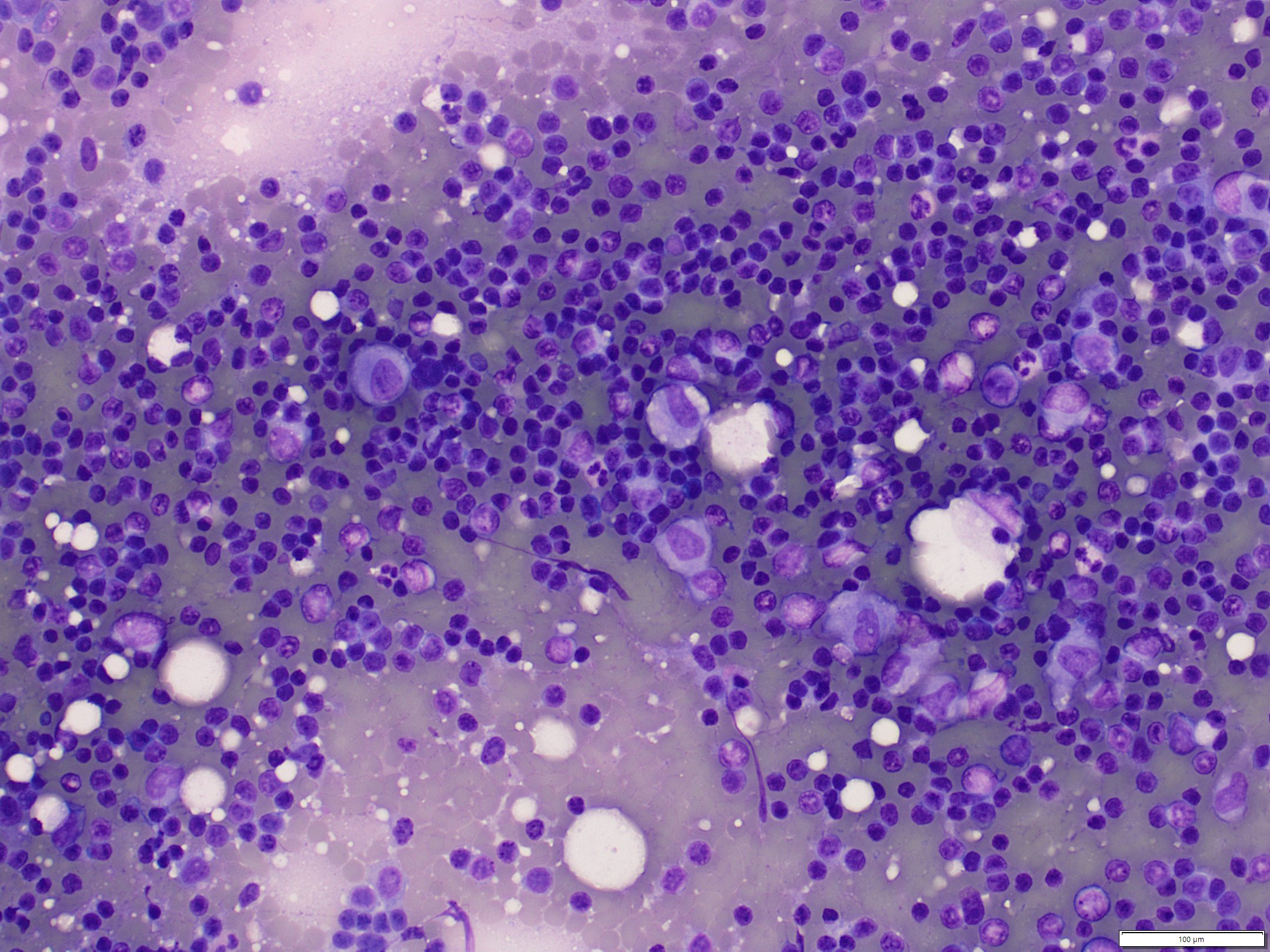
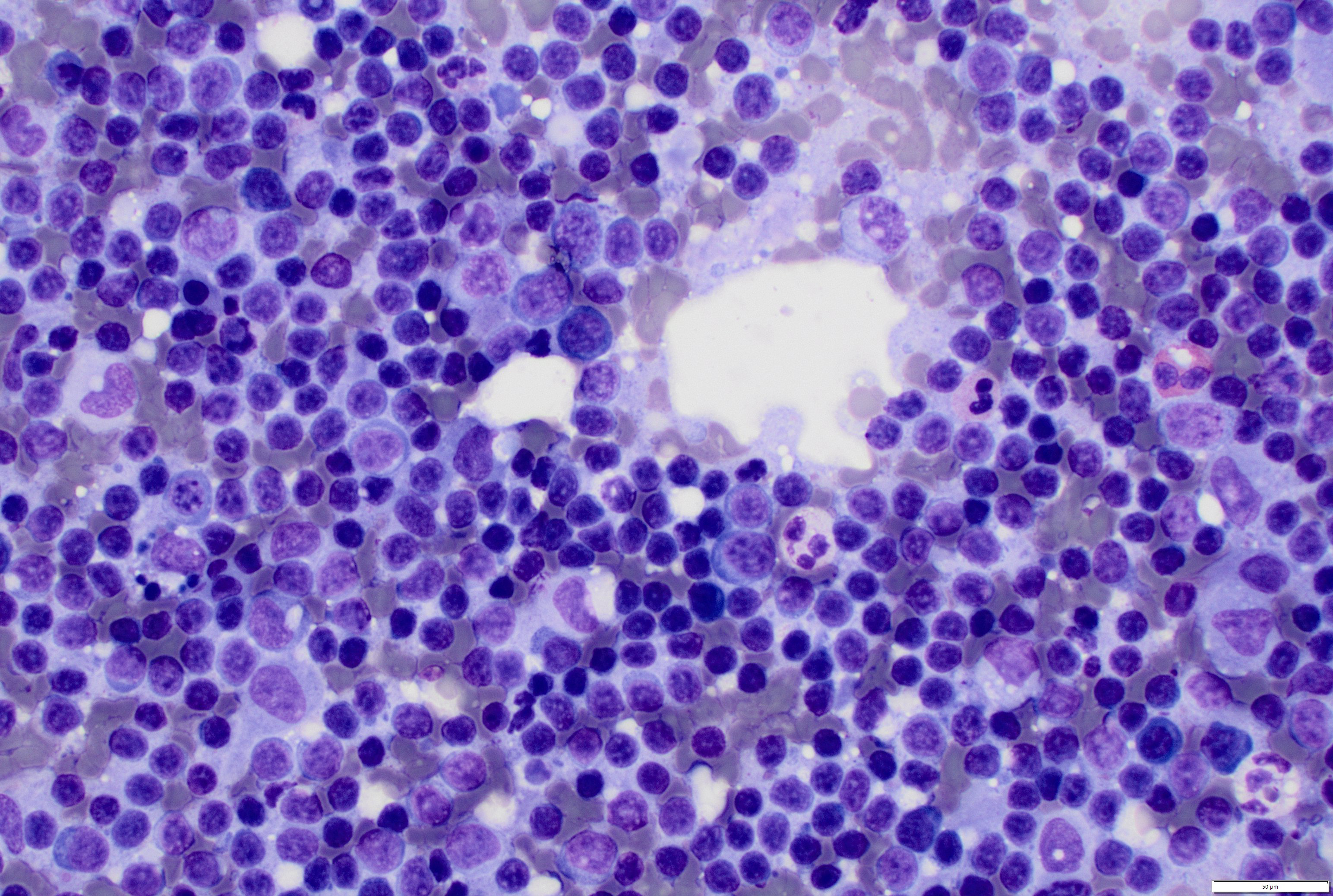
- Figure 1-4: Touch preparation, Diff-Quik stain, 100x (Fig 1), 200x (Fig 2-3), 400x (Fig 4)
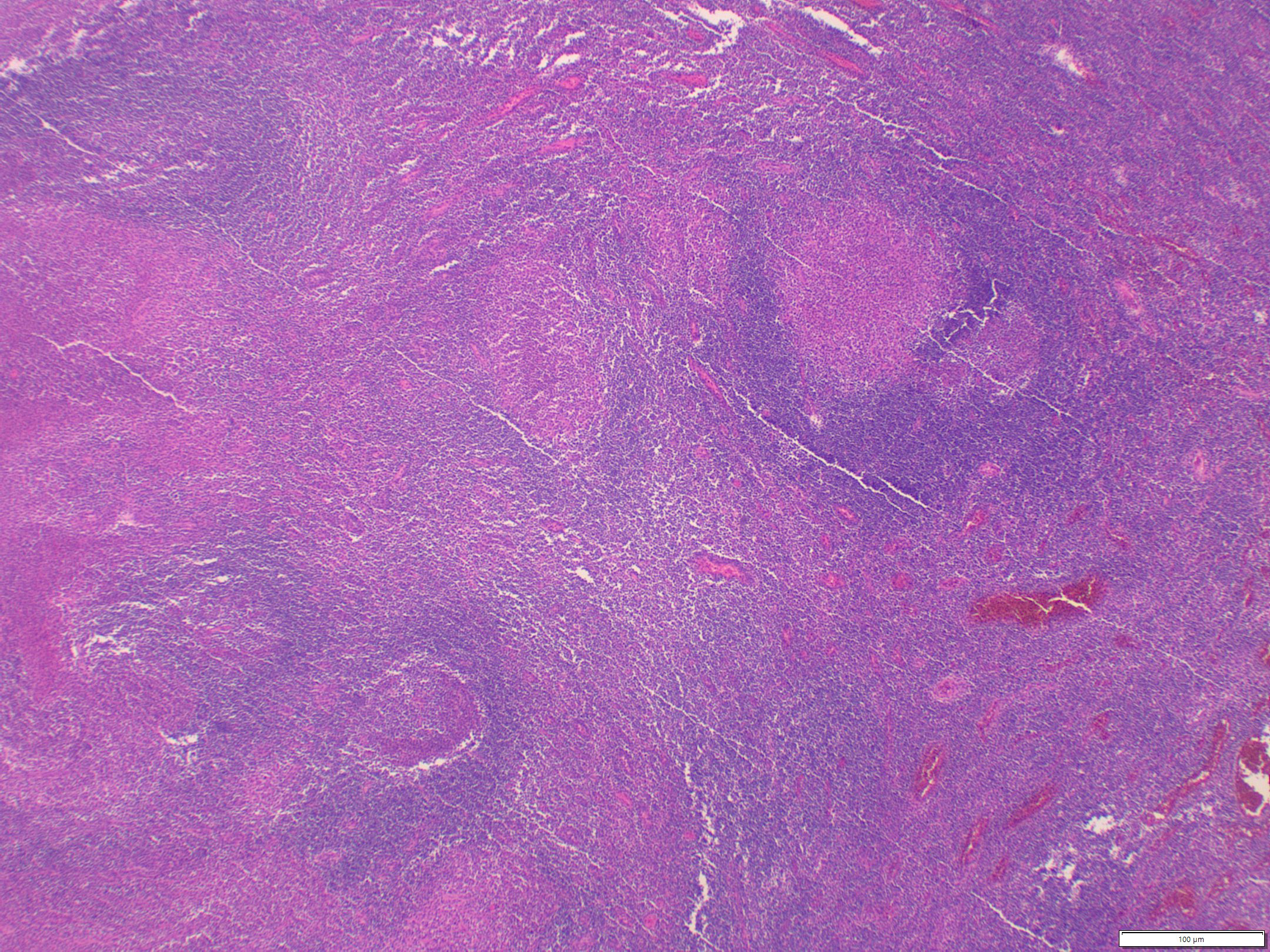
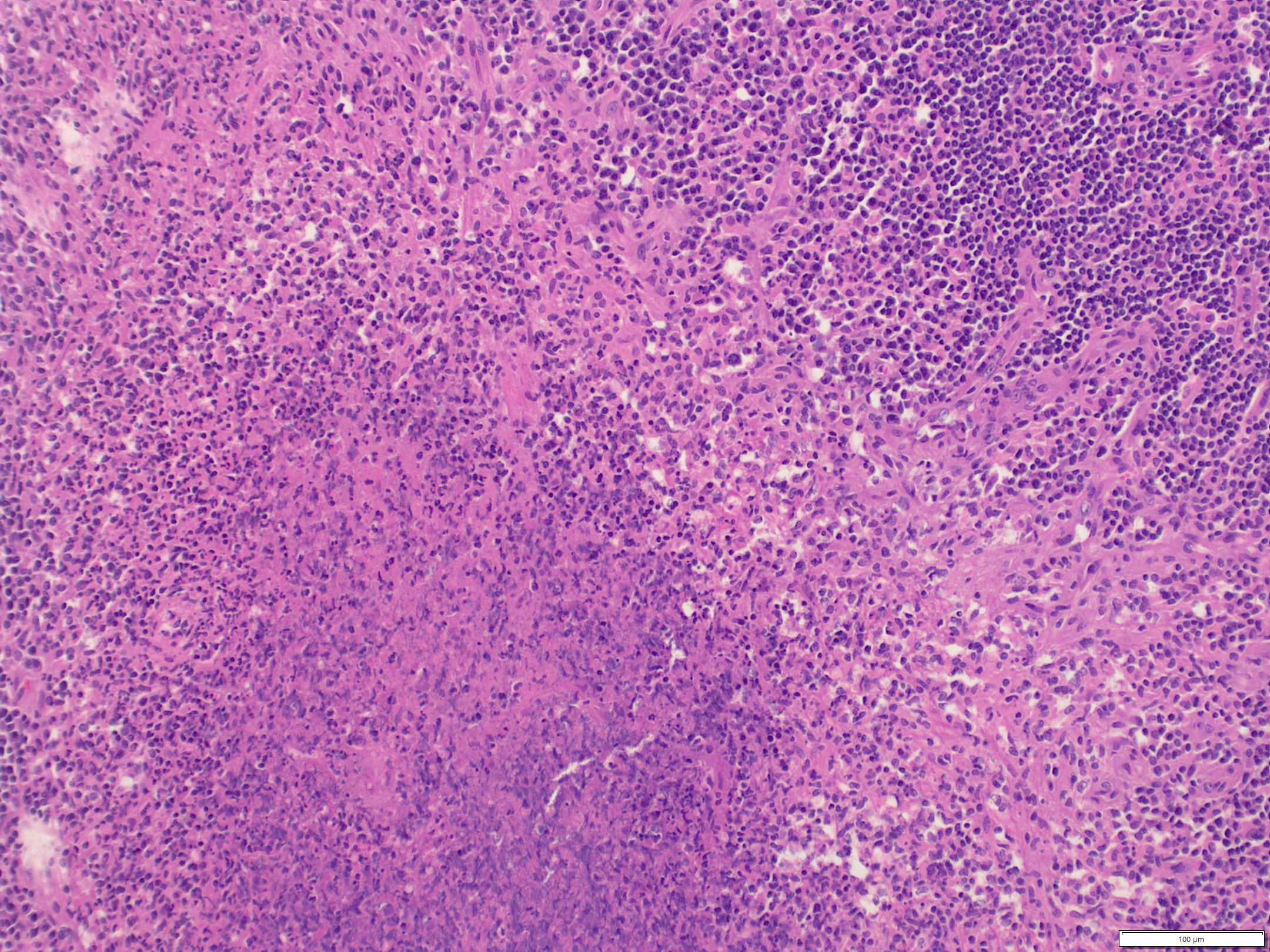
- Figure 5-6: Histology of the lymph node, H&E stain, 20x, 100x, respectively
Questions:
- Based on the information given, which of the following is the most likely diagnosis:
- Necrotizing granulomatous lymphadenitis consistent with cat-scratch disease (CSD)
- Sarcoidosis
- Lymphoma
- Kimura disease
- An immunocompromised patient develops bacillary angiomatosis and peliosis hepatis. Which of the following is biologically, phylogenetically, and morphologically most related to the organism responsible for this patient's condition?
- Rickettsia prowazekii
- Bartonella henselae
- Tropheryma whipplei
- Chlamydia trachomatis
- Leishmania donovani
- The histopathologic evolution of cat scratch disease progresses through characteristic stages. Which of the following represents the correct temporal sequence?
- Stellate microabscesses -> follicular hyperplasia -> granulomatous inflammation
- Follicular hyperplasia with histiocytic proliferation -> granulomatous changes -> stellate microabscesses
- Granulomatous inflammation -> follicular hyperplasia -> fibrosis
- Caseous necrosis -> non-necrotizing granuloma -> follicular hyperplasia
- Which of the following statements best compares the utility of the Warthin-Starry stain to Polymerase Chain Reaction (PCR) on tissue sample?
- Warthin-Starry has a higher sensitivity than PCR but lacks the ability to differentiate Bartonella species from other silver-reducing artifacts
- PCR provides superior specificity by utilizing species-specific primers, whereas Warthin-Starry is prone to false positives caused by tissue precipitates and reticulin fibers
- Both Warthin-Starry and PCR preserve the spatial and structural architecture of the microabscesses to directly correlate bacterial load with tissue morphology
- PCR requires fresh, unfixed tissue and cannot be performed on the formalin-fixed, paraffin-embedded (FFPE) blocks used for the Warthin-Starry stain.
Answers:
Question 1: Correct answer is A. Necrotizing granulomatous lymphadenitis consistent with cat-scratch disease
The touch preparation (Figures 1-4) showed polymorphous lymphocytes, abundant neutrophils, increased epithelioid histiocytes and rare other inflammatory cells. Histology sections of the lymph node demonstrated follicular and paracortical hyperplasia, as well as multiple foci of eosinophilic necrosis admixed with numerous neutrophils that formed small abscesses surrounded by epithelioid macrophages (Figures 5-6). Flow cytometry studies detected no significant immunophenotypic abnormalities. No definitive microorganisms were identified with GMS, Gram, and AFB stains. CMV, HSV1/2, and spirochete immunostains were all negative. Serology testing revealed elevated Bartonella henselae IgM and IgG titers, and Bartonella PCR of the lymphoid tissue was positive, confirming the diagnosis of CSD. Upon further inquiry, the patient had a history of cat exposure at home.
The morphology of stellate microabscesses is highly characteristic of cat-scratch disease (CSD), caused by Bartonella henselae. Early lesions exhibit follicular hyperplasia and histiocytic proliferation; advanced changes progress to granulomatous inflammation with varying-sized abscesses, central or stellate necrosis with abundant neutrophils, and a surrounding rim of palisading histiocytes.
Sarcoidosis is characterized by non-caseating (non-necrotizing) epithelioid granulomas that usually do not show suppuration. Lymphoma may present with granulomatous inflammation, but is distinguished by the presence of Reed-Sternberg cells in Hodgkin lymphoma or atypical, mixed, and malignant cells in non-Hodgkin lymphoma. Kimura disease is a chronic inflammatory disorder distinct for its prominent tissue and blood eosinophilic infiltration.
Question 2: Correct answer is B. Bartonella henselae
Both CSD and bacillary angiomatosis (vascular proliferative disease in immunocompromised patients) are caused by Bartonella henselae. Peliosis hepatis (blood-filled cystic spaces in the liver) is another manifestation of Bartonella infection in the immunocompromised.
Question 3: Correct answer is B. Follicular hyperplasia with histiocytic proliferation -> granulomatous changes -> stellate microabscesses
Early lesions of CSD have follicular hyperplasia and histiocytic proliferation, intermediate lesions have granulomatous changes, and late lesions have abscesses of various sizes with central necrosis surrounded by palisading histiocytes. The progression is important for pathologists to recognize, as biopsy of early stages may lack the classic suppurative granulomas.
Question 4: Correct answer is B. PCR provides superior specificity by utilizing species-specific primers, whereas Warthin-Starry is prone to false positives caused by tissue precipitates and reticulin fibers.
Bartonella henselae is difficult to distinguish from background artifacts (such as melanin, nerve fibers, or silver chemical precipitation) on a Warthin-Starry stain, leading to low specificity. PCR targets specific genomic sequences, providing definitive species-level identification and the highest diagnostic specificity. PCR has significantly higher sensitivity compared to the Warthin-Starry stain. PCR requires tissue homogenization, which completely destroys tissue architecture and eliminates spatial context. Modern PCR assays are routinely and successfully performed on DNA extracted directly from FFPE tissue blocks.
REFERENCES:
- Medeiros LJ, Roberto N. Miranda RN. Diagnostic Pathology: Lymph Nodes and Extranodal Lymphomas, 3rd Edition, page 52-57
- Sabir S, Daley SF, Huang B. Cat Scratch Disease. [Updated 2025 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482139/