Case of the Month ...

A 23-year-old pregnant female presented with a large mediastinal mass involving the right hilum and pulmonary vasculature. Imaging revealed an aggressive infiltrative lesion with mediastinal lymphadenopathy. Endobronchial ultrasound-guided fine needle aspiration (EBUS-FNA) of lymph node station 7 was performed for initial diagnosis. Cytology smears, cell block material and representative immunohistochemical stains are below. Not pictured are TTF1, synaptophysin, INSM1 and D2-40, which were negative within tumor cells and SMARCB1/INI1 (intact).
Authors
- Arkar Htoo, MD, FCAP. Head and Neck Molecular Cytopathology, Henry Ford Health (Cleveland Clinic Foundation – previous institution)
- Marko Golusin, MD, FCAP. Cytopathology, Robert J. Tomsich Department of Pathology & Laboratory Medicine, Diagnostic Institute, Cleveland Clinic Foundation
click on image for larger version
Figure 3 Figure 4 Figure 5 Figure 6 Images 1-6:
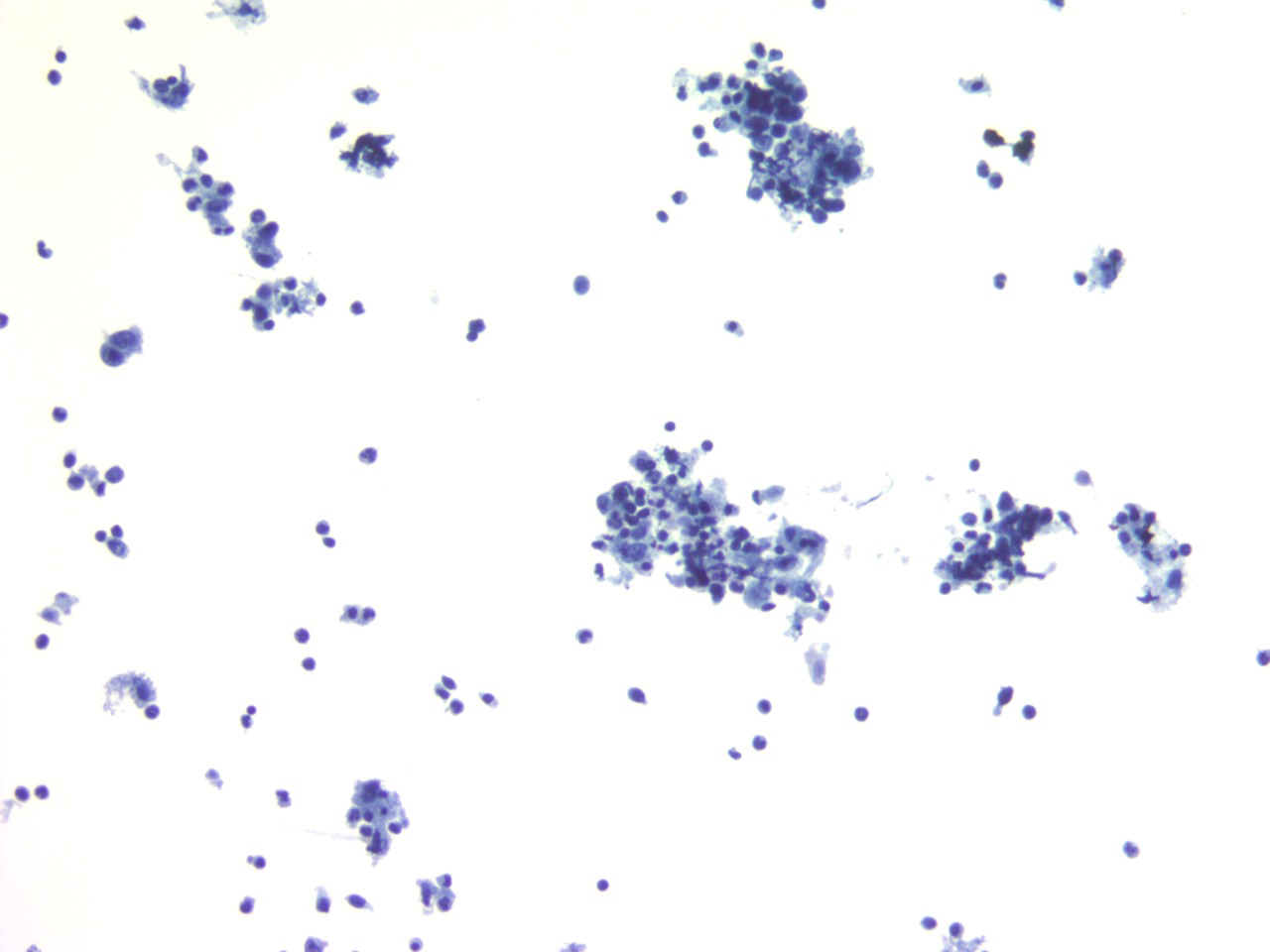
- Figure 1: Transbronchial FNA of station 7 lymph node, aspirate smear, ThinPrep, 20× magnification.
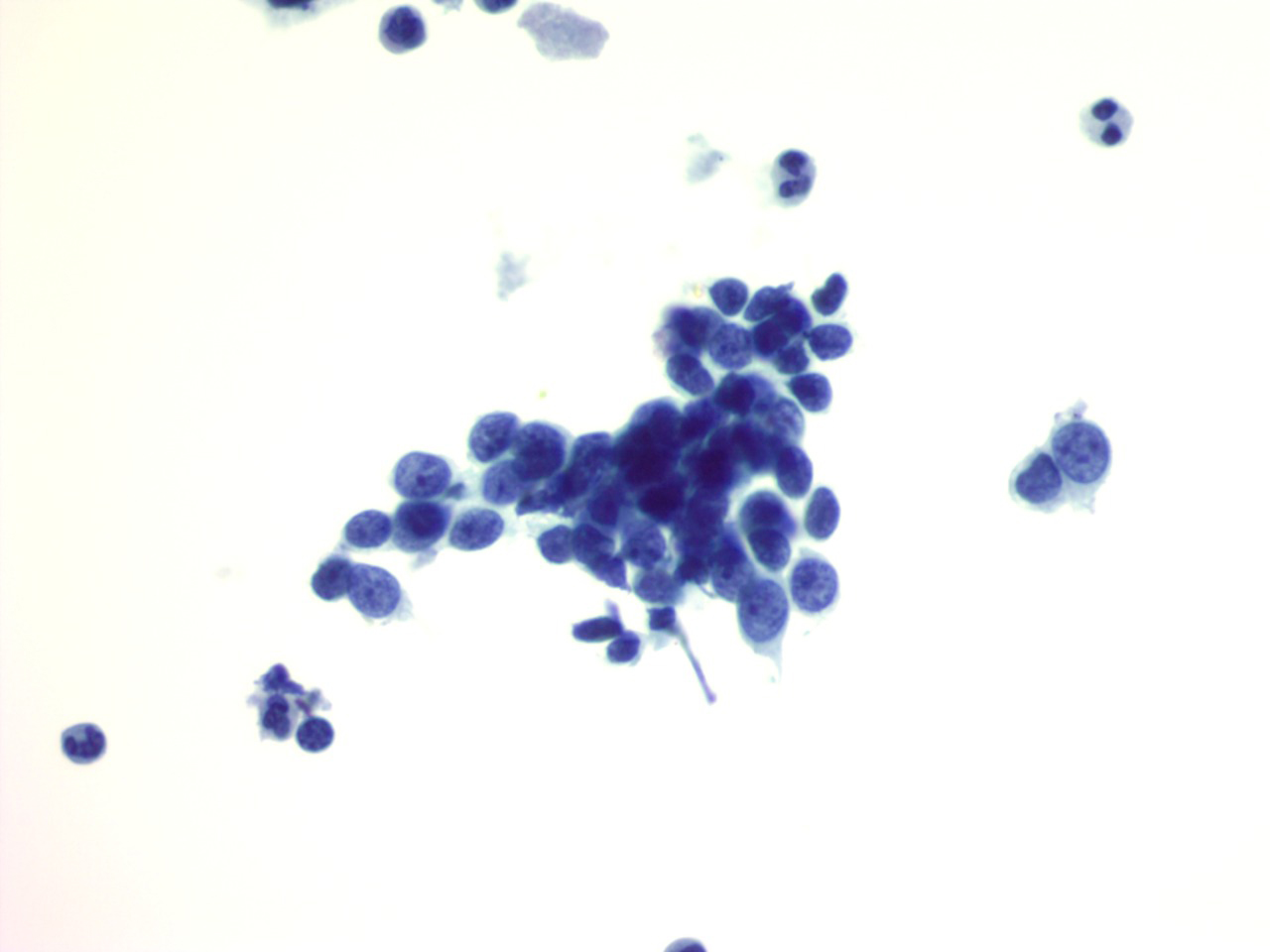
- Figure 2: Transbronchial FNA of station 7 lymph node, aspirate smear, ThinPrep, 40× magnification.
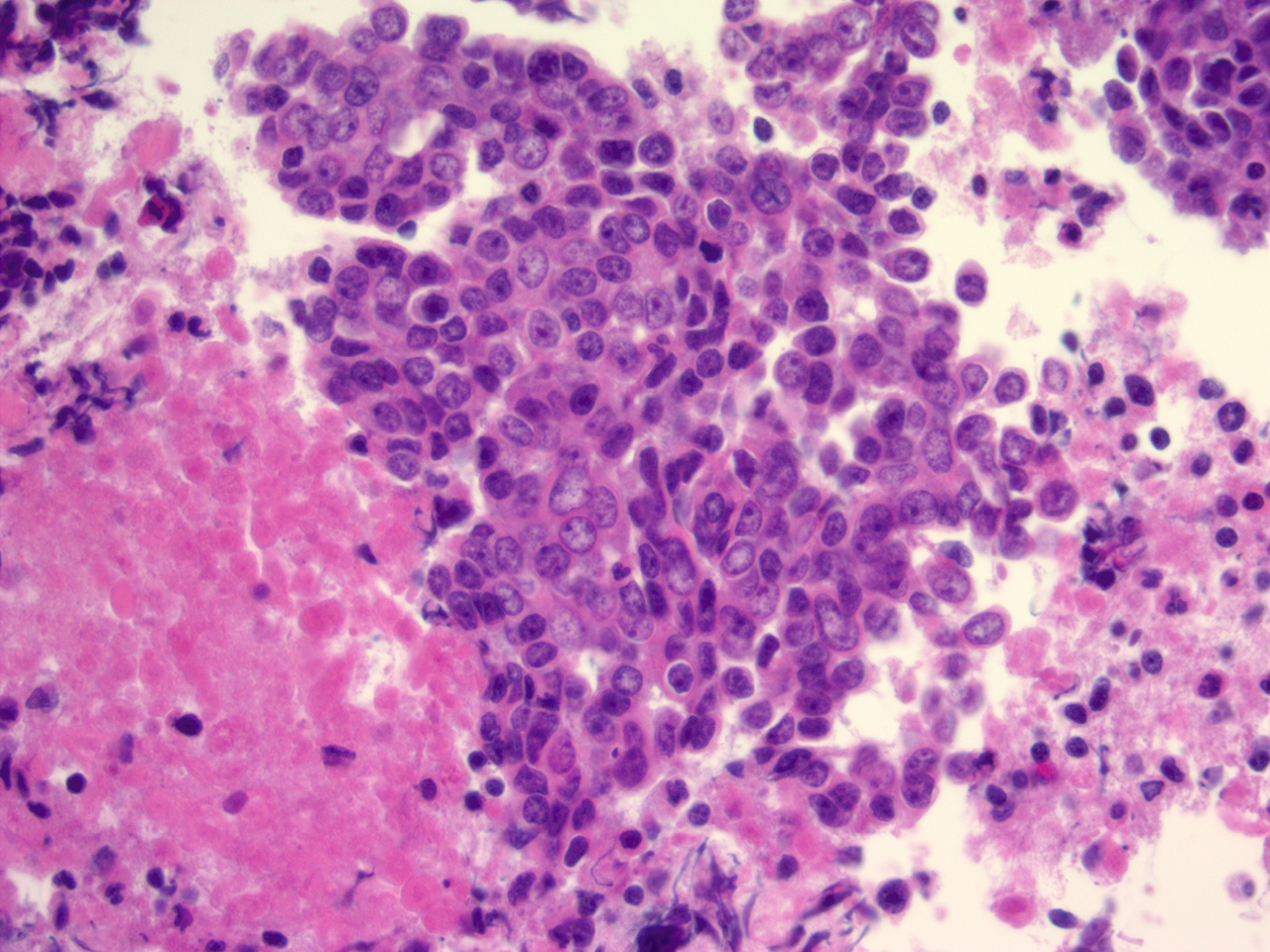
- Figure 3: Cell block, H&E stain, 40× magnification.
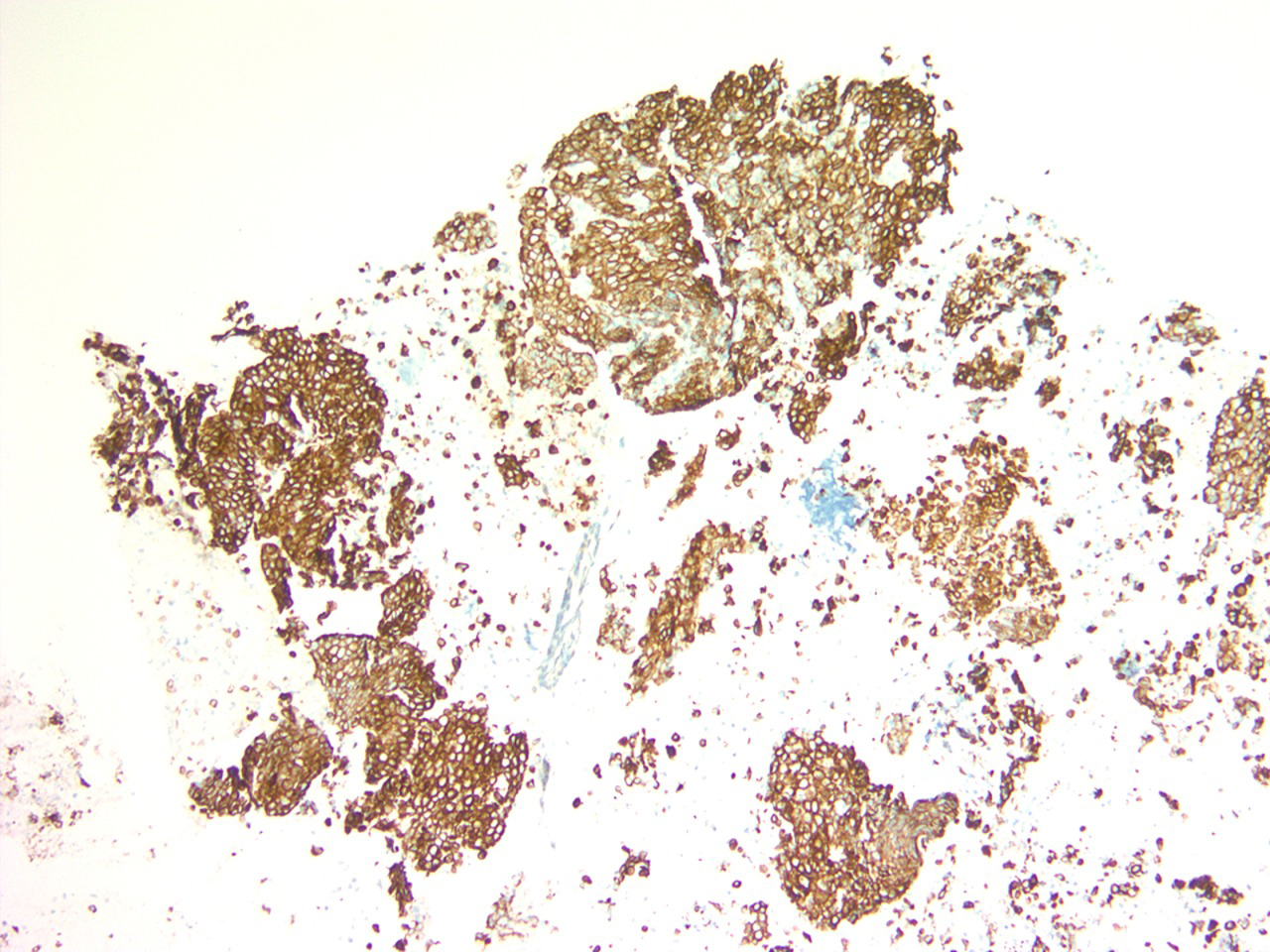
- Figure 4: Cell block, CAM 5.2 immunohistochemical stain, 10× magnification.
- Figure 5: Cell block, p40 immunohistochemical stain, 10× magnification.
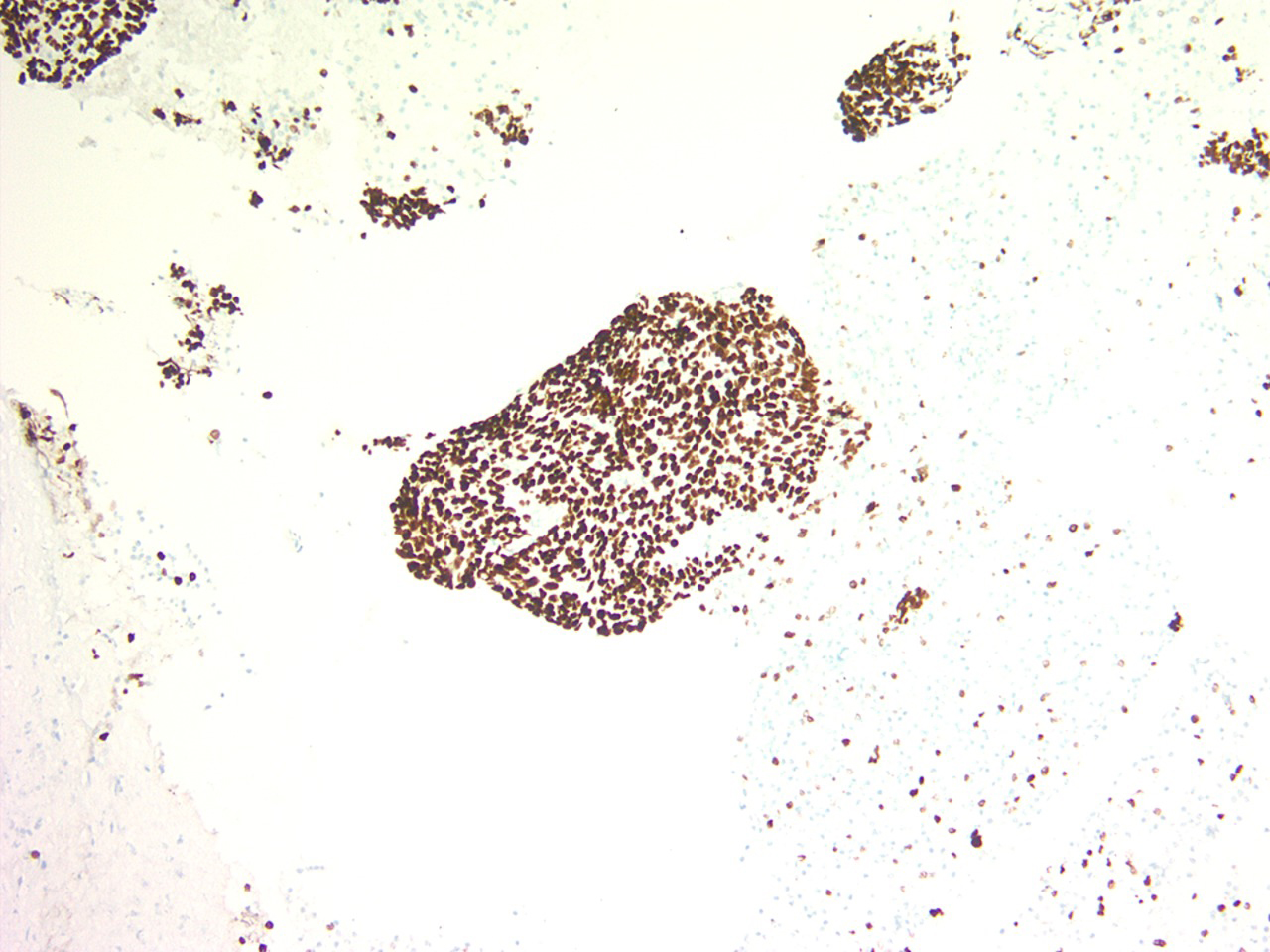
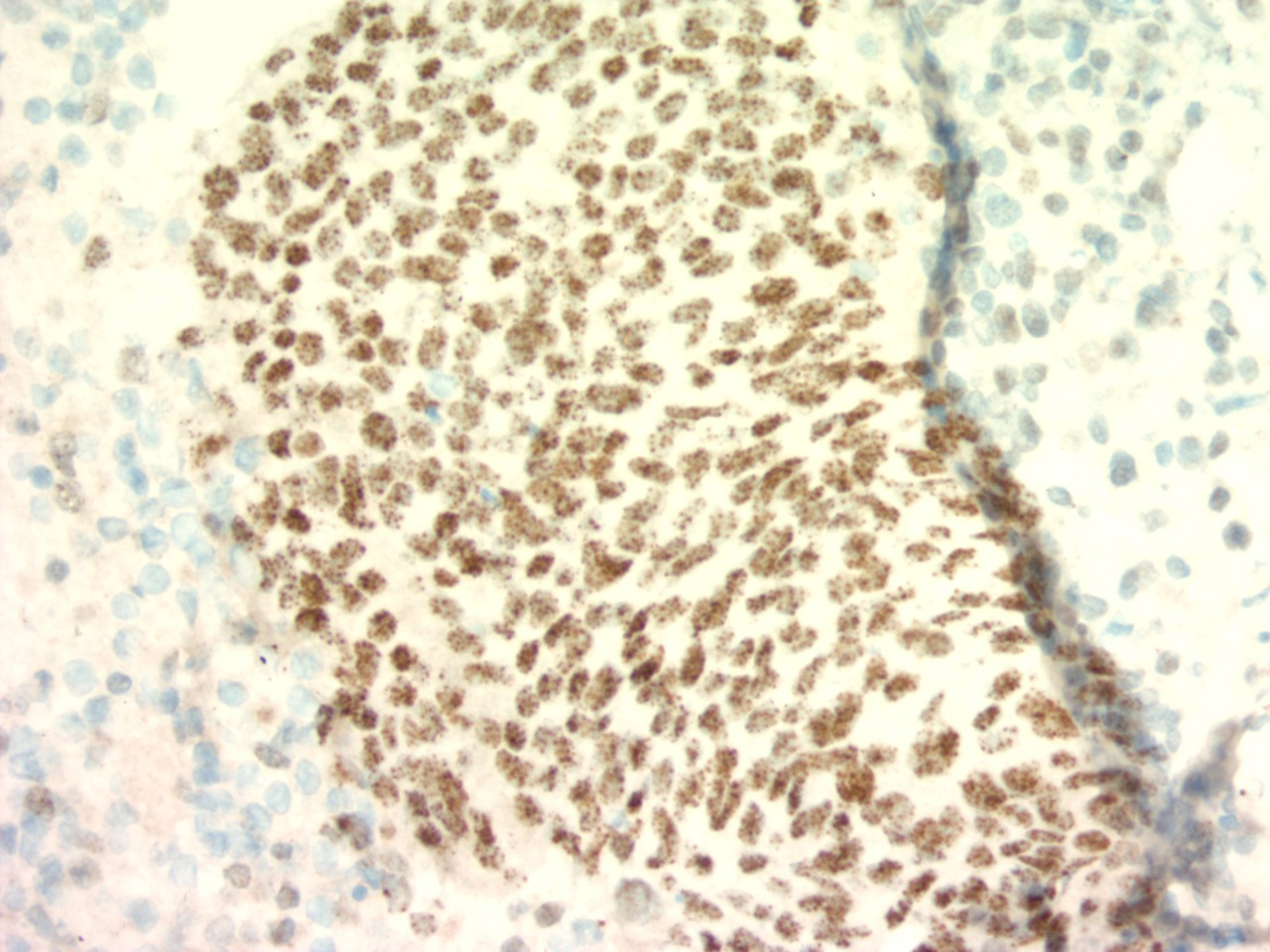
- Figure 6: Cell block, NUT immunohistochemical stain, 40× magnification.
Questions:
- Based on cytomorphology, immunohistochemistry, and clinical information, what is the correct diagnosis for this patient?
- Small cell carcinoma
- Poorly differentiated squamous cell carcinoma
- NUT carcinoma
- Lymphoma
- SMARCA4-deficient undifferentiated tumor
- Which immunohistochemical finding is most characteristic and essentially diagnostic in this entity?
- Diffuse cytoplasmic synaptophysin positivity
- Loss of INI1 expression
- Strong diffuse TTF-1 positivity
- Speckled nuclear staining with NUT antibody
- Diffuse CD45 positivity
- What is the most common underlying molecular alteration in this tumor?
- EWSR1-FLI1 fusion
- BRD4-NUTM1 fusion
- ALK rearrangement
- EGFR exon 19 deletion SMARCB1 deletion
Answers:
Question 1: Correct answer is C. NUT carcinoma
Cytomorphology shows a highly cellular specimen composed of a poorly differentiated malignant neoplasm with extensive necrosis. The tumor cells are present singly and in loosely cohesive clusters, medium to large in size with scant to moderate cytoplasm, irregular nuclear contours, vesicular nuclear chromatin, and prominent nucleoli. The background shows abundant necrosis and apoptotic debris. Abrupt squamous differentiation is a well-recognized morphologic feature of NUT carcinoma; however, this feature was not well developed in this case.1
Immunohistochemistry demonstrates epithelial differentiation (AE1/AE3, CAM5.2) and squamous differentiation (p40, p63). The tumor cells are negative for TTF-1, synaptophysin, INSM1, D2-40, CD3, CD20, calretinin, and SOX10. Flow cytometry is negative. Crucially, the tumor shows diffuse nuclear positivity for NUT with a speckled staining pattern, which is diagnostic of NUT carcinoma.2
Option A. Small cell carcinoma: Typically shows nuclear molding, finely granular (“salt-and-pepper”) chromatin, scant cytoplasm, and high mitotic activity. Immunohistochemically, it is positive for neuroendocrine markers such as synaptophysin and INSM1, which are negative in this case.
Option B. Poorly differentiated squamous cell carcinoma: Can show overlapping morphology and positivity for p40 and p63; however, it lacks NUT nuclear staining and typically occurs in older patients with smoking history. The presence of NUT positivity excludes conventional squamous cell carcinoma.
Option D. Lymphoma: Excluded by negative flow cytometry and lack of expression of lymphoid markers (CD45, CD3, CD20). Cytomorphology also does not support a lymphoproliferative process.
Option E. SMARCA4-deficient undifferentiated tumor: Typically demonstrates loss of SMARCA4 (BRG1) expression and often loss of Rb1. These tumors frequently lack strong squamous marker expression. In this case, Rb1 expression is retained, and the tumor expresses p40/p63, arguing against this entity.
Question 2: Correct answer is D. Speckled nuclear staining with NUT antibody
Diffuse (>50%) nuclear staining for NUT immunohistochemistry, typically with a speckled pattern, is 100% specific and approximately 87% sensitive for a diagnosis of NUT carcinoma. Immunohistochemical positivity for NUT serves as a surrogate marker for the presence of a NUTM1 fusion protein. The combination of NUT immunohistochemistry and FISH for NUT rearrangements increases the diagnostic sensitivity to 100%. In the appropriate morphologic and clinical context, these findings are highly specific and diagnostic.2
Option A. Diffuse cytoplasmic synaptophysin positivity: Indicates neuroendocrine differentiation and would support small cell carcinoma or other neuroendocrine tumors, which are excluded in this case by negative synaptophysin and INSM1 staining.
Option B. Loss of INI1 expression: Seen in SMARCB1-deficient tumors such as epithelioid sarcoma or malignant rhabdoid tumor, not in NUT carcinoma.
Option C. Strong diffuse TTF-1 positivity: Characteristic of pulmonary adenocarcinoma and some small cell carcinomas; TTF-1 is negative in this case.
Option E. Diffuse CD45 positivity: Indicates a hematolymphoid neoplasm (e.g., lymphoma), which is excluded by immunohistochemistry and flow cytometry in this case.
Question 3: Correct answer is B. BRD4-NUTM1 fusion
NUT carcinoma is molecularly defined by rearrangements involving the NUTM1 gene, most commonly resulting in a BRD4-NUTM1 fusion, which accounts for approximately 70–80% of cases.3 This fusion leads to the formation of an oncogenic protein that drives aberrant transcription and blocks differentiation, contributing to the aggressive clinical behavior of these tumors.Clinically, NUT carcinoma is a rare but highly aggressive malignancy that typically arises in midline structures such as the mediastinum and affects younger patients. Recognition is critical, as emerging targeted therapies, including bromodomain and extraterminal (BET) inhibitors, may offer therapeutic benefit.3
The cytologic findings in this case including a highly cellular aspirate with discohesive malignant cells, necrotic background on Diff-Quik and Papanicolaou smears, and poorly differentiated carcinoma on cell block together with the characteristic immunophenotype and molecular alteration, are diagnostic of NUT carcinoma.
Option A. EWSR1-FLI1 fusion: Characteristic of Ewing sarcoma, a small round blue cell tumor that lacks epithelial and squamous marker expression and does not show NUT positivity.
Option C. ALK rearrangement: Seen in a subset of lung adenocarcinomas and inflammatory myofibroblastic tumors; these tumors typically express TTF-1 (in lung adenocarcinoma) and lack NUT staining.
Option D. EGFR exon 19 deletion: A common driver mutation in lung adenocarcinoma, which would show glandular differentiation and TTF-1 positivity, not seen here.
Option E. SMARCB1 deletion: Seen in SMARCB1-deficient tumors such as malignant rhabdoid tumor; these tumors demonstrate loss of INI1 expression, which is not a feature of NUT carcinoma.REFERENCES:
- Luo, J., Bishop, J.A., DuBois, S.G. et al. Hiding in plain sight: NUT carcinoma is an unrecognized subtype of squamous cell carcinoma of the lungs and head and neck. Nat Rev Clin Oncol 22, 292–306 (2025). https://doi.org/10.1038/s41571-025-00986-3
- Wang S, Li J, Tong W, Li H, Feng Q, Teng B. Advances in the pathogenesis and treatment of nut carcinoma: a narrative review. Transl Cancer Res. 2020;9(10):6505-6515. doi:10.21037/tcr-20-1884
- Zhang Y, Zhang Q, Hao Y, et al. International guidelines on the diagnosis and treatment of NUT carcinoma. Innovation (Camb). 2025;7(1):101068. Published 2025 Jul 31. doi:10.1016/j.xinn.2025.101068
- Haack H, Johnson JA, Fry CJ, et al. Diagnosis of NUT midline carcinoma using a NUT-specific monoclonal antibody. Am J Surg Pathol. 2009;33(7):984-991. PMID: 19363441